Examining Treatment Options for Second-Line ES-SCLC Therapy
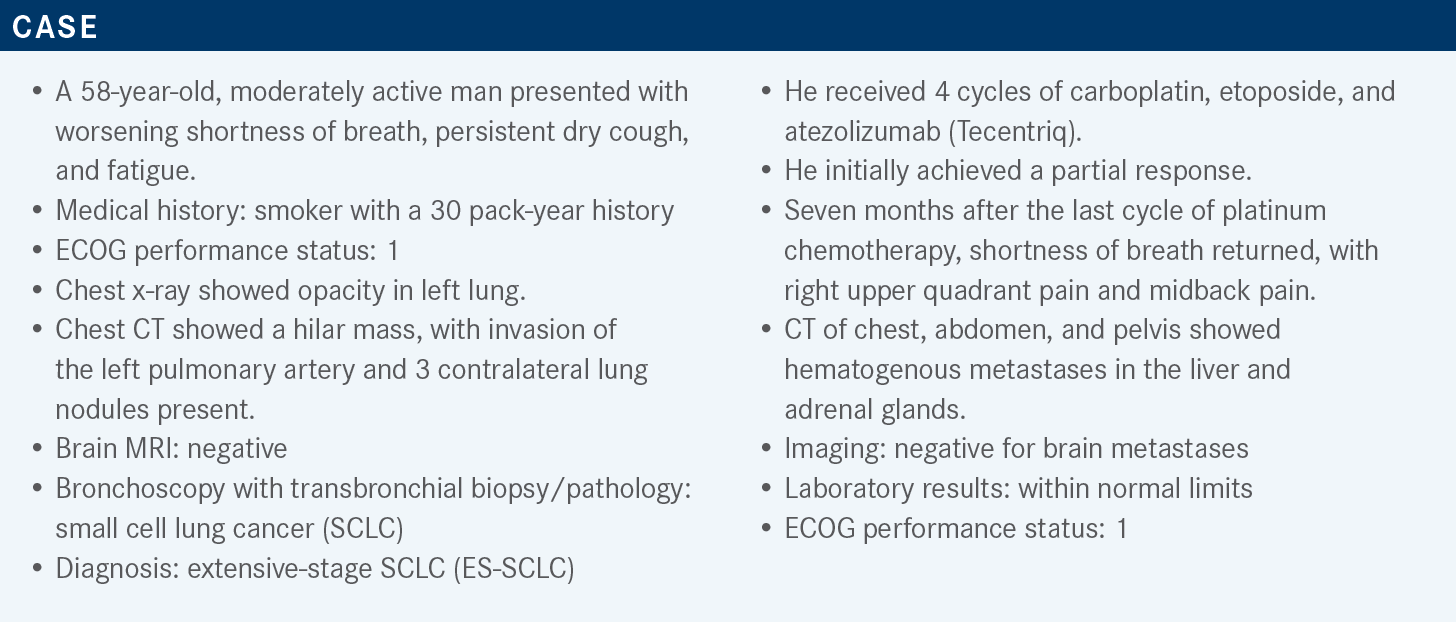
During a Targeted Oncology case-based roundtable event, Rafael Santana-Davila, MD, discussed the data supporting the use of immunotherapy for patients with extensive-stage small cell lung cancer.



Rafael Santana-Davila, MD
Associate Professor
Clinical Research Division
Fred Hutchinson Cancer Research Center
Associate Professor, Medicine and Oncology
University of Washington School of Medicine
Medical Director, Infusion and Pharmacy Services
Seattle Cancer Care Alliance


Targeted OncologyTM: What is the recommended second-line therapy for ES-SCLC?
SANTANA-DAVILA: The National Comprehensive Cancer Network [NCCN] guidelines on SCLC recommend that if [the relapse occurs within] 6 months, the options are either oral or intravenous (IV) topotecan, lurbinectedin [Zepzelca], or a clinical trial.1 [Other recommended regimens are] taxanes, irinotecan [Camptosar], temozolomide [Temodar] in the presence of brain disease especially, and CAV [cyclophosphamide (Cytoxan), doxorubicin (Adriamycin), vincristine (Oncovin)] chemotherapy.
Bendamustine [Treanda] is category 2B because it showed some activity in a clinical trial. In patients who have relapsed for more than 6 months after initial therapy, the recommendation is to give the original regimen. Lurbinectedin is the only drug that has been approved [recently], and this was in June 2020.2
What data support a platinum rechallenge?
The NCCN panel recommends rechallenge for relapse after 6 months [from treatment]. There’s another study that was published in Lancet in 2020.3 This was a French study. In France, and Europe in general, they use 90 days to define platinum sensitivity, and this was a study where patients with SCLC who have progressed at least 90 days [after completion of first-line treatment] were [randomly assigned] to topotecan or platinum rechallenge. Interestingly, the median progression-free survival [PFS] was better in patients who were rechallenged with platinum at 4.7 months vs 2.7 months in patients treated with topotecan [HR, 0.57; 90% CI, 0.41- 0.73; P = .0041].3
There was a larger overall response rate [ORR] difference. It was 49% for platinum therapy vs 25% for topotecan [P = .0024]. Interestingly though, it’s not clear that overall survival [OS] was changed. But if we look at the trial, up to one-third of patients who were [randomly assigned] to topotecan went on to receive third-line platinum rechallenge. One might suspect that is the reason why they did not show an OS advantage.3
In my practice, if a patient had a decent tolerance to a platinum challenge and it’s been more than 3 months, based on these data, I consider rechallenging with the same platinum agent. I typically use a platinum and a taxane, just because there’s nothing magical about etoposide for this traditionally. My idea is because this is platinum rechallenge, it is best to introduce a second agent that tends to be as equally tolerated as etoposide without having them come [to the clinic] for a few days straight. I typically do that as a standard in patients that have a platinum rechallenge after 90 days. A lot has to do with how they tolerate treatment and what their goals are. If the platinum rechallenge beats them up, I tend to go to a single agent. So to me these goals are obviously important.
Why is immuno-oncology (IO) not considered an option for these patients, considering data showing efficacy of ipilimumab (Yervoy) and nivolumab (Opdivo)?
If patients relapse while on maintenance IO, I think that they’ve proven that it does not work, and I do not rechallenge them. Back before the era of immunotherapy, there was [the CheckMate 032] phase 1/2 study [NCT01928394] that showed patients who had progressive disease after chemotherapy who were treated with ipilimumab or nivolumab. [Some cohorts were] nonrandomized.
Some patients were treated with nivolumab alone. Some patients were treated with high-dose ipilimumab at 3 mg/m2 and low-dose nivolumab at 1 mg/m2, and the other way around. They found that patients who were treated with 3 mg of ipilimumab and 1 mg of nivolumab had a 22% response rate.4 Because of that, the NCCN endorsed that regimen, which lived for a little bit. Then came the atezolizumab and durvalumab [Imfinzi] data, and there was no reason to put patients on ipilimumab or nivolumab if they had already had exposure to immunotherapy.
Then there were 2 clinical trials that were done, 1 in the maintenance setting [NCT01450761] where patients were treated with a platinum-based agent and etoposide. After the 4 cycles, they were randomly assigned to etoposide alone vs etoposide and ipilimumab, which did not show any evidence of improvement in OS for the patients on ipilimumab.5
But it did [result in] toxicity, and this was a higher-dose ipilimumab, [10 mg/kg, which] was significant. The incidence of colitis was high. Similarly, there was another study [CheckMate 451; NCT02538666] that was a phase 3 study where patients on second-line therapy who were immunotherapy naive were randomly assigned to ipilimumab and nivolumab vs nivolumab alone [vs placebo]. There was no evidence of improvement in OS.6 It’s difficult to know why this was the case and why we saw an improvement before, but based on those data, the NCCN decided to not endorse this regimen anymore. I’ve had a couple of patients that are 3 and 5 years out from ipilimumab plus nivolumab when we could do that, and the disease is under control. Were we just lucky? Does ipilimumab have anything to do with it? We don’t know, but unfortunately, we don’t have a role for ipilimumab and nivolumab outside a clinical trial setting.
I would not use [nivolumab and ipilimumab]. I am biased because thankfully I have access to clinical trials. When my patients are on third-line therapy, I would not use it, and I would not recommend it. Is it wrong to use it? No, I don’t think so, but do the data support it? No, they do not.
What data support the use of lurbinectedin for SCLC after progressing with chemotherapy?
Lurbinectedin was approved based on a phase 2 basket study [NCT02454972].2 It’s an interesting story. Lurbinectedin comes from a Spanish company called PharmaMar, [which was] looking at different compounds that were researched at sea and...developed lurbinectedin as one of those compounds. [PharmaMar] first started [lurbinectedin] in a large phase 1 study [NCT01980667] and noticed that a few patients with SCLC responded, so [it] did the basket study using the maximum tolerated dose of lurbinectedin at 3.2 mg/m2 IV every 3 weeks. [It] also did the ATLANTIS study [NCT02566993], which is a phase 3 study of lurbinectedin. [PharmaMar] didn’t think that lurbinectedin alone would control the disease, so [it] used lurbinectedin and doxorubicin compared with topotecan or CAV, which is commonly used in Europe. [It] did these 2 studies in parallel.
The basket study was presented first at the 2018 American Society of Clinical Oncology Annual Meeting and was later published in Lancet in 2020.7 It was a single-arm study in patients that had an ECOG performance score of 0 to 2 and prior chemotherapy exposure. Prior immunotherapy was allowed; it was still not the standard of care. Patients with CNS [central nervous system] metastases were excluded, and the primary end point was the ORR. The null hypothesis was a 15% or less response, and the alternative hypothesis was a response of more than 30%.7
So 105 patients were treated with this regimen, more men than women—as is seen in the disease commonly. The median age was 60. Most patients had an ECOG status of 0 or 1. Only 8 did not. Most were smokers, as you might expect. CNS involvement was present in 4%. Again, they did not have active brain metastases. Patients who had treated brain metastases were allowed. For prior therapies, platinum was used in 100% of the cases, etoposide in 99%, IO in 8%, and PARP inhibitors in 2%. The important thing to note is IO is only in 8% of the cases. That is because this was not the standard of care then. Prior response to platinum was what we would expect. The majority of patients had a partial response at 67%. Complete response [CR] was 9%, and stable disease [SD] was 18%. Forty-three percent of patients had a median chemotherapy-free interval [CTFI] of less than 90 days, and 57% of patients had a CTFI of more than 90 days.7
What was the efficacy seen in this trial?
In all patients, the ORR was 35.2% [95% CI, 26.2%- 45.2%]. There were no CRs, and 33% had SD [for at least] 3 months.7 Progressive disease was present in 27% of the patients. The disease control rate was 68.6%, and the median duration of response was 5.3 months, with 43% of patients still responding at 6 months. The median follow-up was 17.1 months.
Patients who had a CTFI of less than 90 days obviously had worse and more aggressive disease [Table7]. The median PFS in these patients was 2.6 months vs 4.6 months in those who had an interval of more than 90 days. The 4-month PFS rate was 29.1% in the less-than-90-days [CTFI] group vs 59.9% in the more-than-90-days [CTFI] group. The 6-month PFS rate was 18.8% in the less-than-90- days group vs 43.5% in the more-than-90-days group. The median OS was 5.0 months in the less-than-90-days group vs 11.9 months in the more-than-90-days CTFI group.

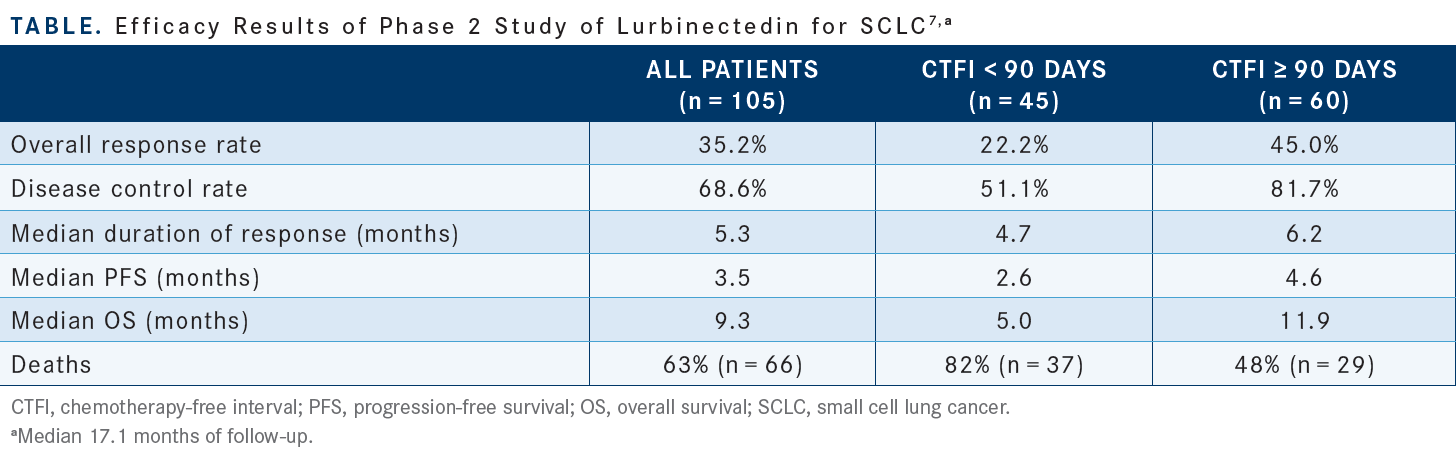
The 12-month OS rate was 15.9% in the less-than-90-days group vs 48.3% in the more-than-90-days group. The ORR in patients with more than 90 days CTFI was 45%, and in patients with more than 180 days, CTFI was 60%.8 The longer patients went without progression, the more likely they had chemotherapy-sensitive disease.
[This regimen] is chemotherapy, so one is going to see adverse effects typical of chemotherapy, including anemia, neutropenia, thrombocytopenia, and fatigue.7 Most of these are grade 1 and 2, but then there is grade 3 fatigue. There was 2% grade 3 and 3% grade 4 febrile neutropenia. This is clearly [consistent with] chemotherapy. The ATLANTIS study had patients randomly assigned to a combination of lurbinectedin and doxorubicin vs topotecan or CAV. It was a negative study, and it is very difficult to know what to make of [those] data because [the study] used low-dose lurbinectedin at only 2 mg/m2.
Had they done their study with single-agent lurbinectedin, would that be a positive study? We don’t know that [yet. Their confirmatory study, LAGOON (NCT05153239), is currently ongoing in the United States and other countries]. We’ll know the data in a few years.
REFERENCES
1. NCCN. Clinical Practice Guidelines in Oncology. Small cell lung cancer, version 2.2022. Accessed July 13, 2022. https://bit.ly/2JTv4zC
2. FDA grants accelerated approval to lurbinectedin for metastatic small cell lung cancer. FDA. Updated June 16, 2020. Accessed July 13,2022. https://bit. ly/3aGy56x
3. Baize N, Monnet I, Greillier L, et al; Groupe Français de Pneumo-Cancérologie 01–13 investigators. Carboplatin plus etoposide versus topotecan as second-line treatment for patients with sensitive relapsed small-cell lung cancer: an open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2020;21(9):1224-1233. doi:10.1016/S1470-2045(20)30461-7
4. Ready NE, Ott PA, Hellmann MD, et al. Nivolumab monotherapy and nivolumab plus ipilimumab in recurrent small cell lung cancer: results from the CheckMate 032 randomized cohort. J Thorac Oncol. 2020;15(3):426-435. doi:10.1016/j. jtho.2019.10.004
5. Reck M, Luft A, Szczesna A, et al. Phase III randomized trial of ipilimumab plus etoposide and platinum versus placebo plus etoposide and platinum in extensive-stage small-cell lung cancer. J Clin Oncol. 2016;34(31):3740-3748. doi:10.1200/ JCO.2016.67.6601
6. Owonikoko TK, Park K, Govindan R, et al. Nivolumab and ipilimumab as maintenance therapy in extensive-disease small-cell lung cancer: CheckMate 451. J Clin Oncol. 2021;39(12):1349-1359. doi:10.1200/JCO.20.02212
7. Trigo J, Subbiah V, Besse B, et al. Lurbinectedin as second-line treatment for patients with small-cell lung cancer: a single-arm, open-label, phase 2 basket trial. Lancet Oncol. 2020;21(5):645-654. doi:10.1016/S1470-2045(20)30068-1
8. Subbiah V, Paz-Ares L, Besse B, et al. Antitumor activity of lurbinectedin in second-line small cell lung cancer patients who are candidates for re-challenge with the first-line treatment. Lung Cancer. 2020;150:90-96. doi:10.1016/j. lungcan.2020.10.003



















