Roundtable Discussion: Reviewing Management Options for a Patient With TNBC
During a Targeted Oncology case-based roundtable event, Alison K. Conlin, MD, discussed with participants their choice of first- and second-line therapy for a patient with triple-negative breast cancer.




Oncologist
Providence Cancer Institute Franz Clinic
Portland, OR")
Alison K. Conlin, MD (Moderator)
Oncologist
Providence Cancer Institute Franz Clinic
Portland, OR






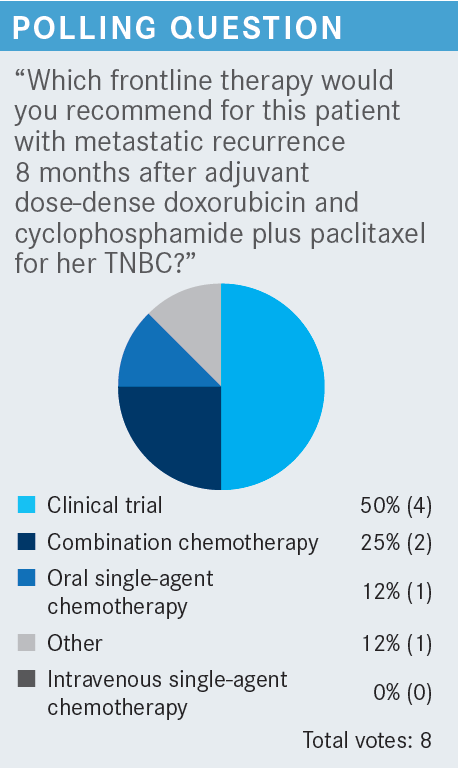
CONLIN: Half of us picked clinical trial, so maybe we have some great clinical trials for these patients. A quarter of us picked combination chemotherapy, [so I’m] wondering whether people mean some sort of platinum combination?
CHINTAPATLA: Combination chemotherapy—I would think carboplatin plus gemcitabine.
CONLIN: Is the oral single-agent therapy capecitabine?
BORKOWSKI: That’s what I thought.
CONLIN: It’s so recent since her taxane. Were people thinking about another option? Anything special?
CHAUNCEY: I’m coming from the [perspective] that I don’t see a lot of these cases, but this is a lot of chemotherapy up front and it’s only 8 months, so [I would go for] a trial. If you don’t have a trial, then something different.
CONLIN: So you feel like she didn’t have a lot of chemotherapy responsiveness. What else?
CHAUNCEY: She’s young, and she only had 8 months of treatment. A platinum therapy could be different, but how different is it?
CONLIN: That’s a good point. You are trying to think outside the box for her other options, so hopefully a trial in that case.


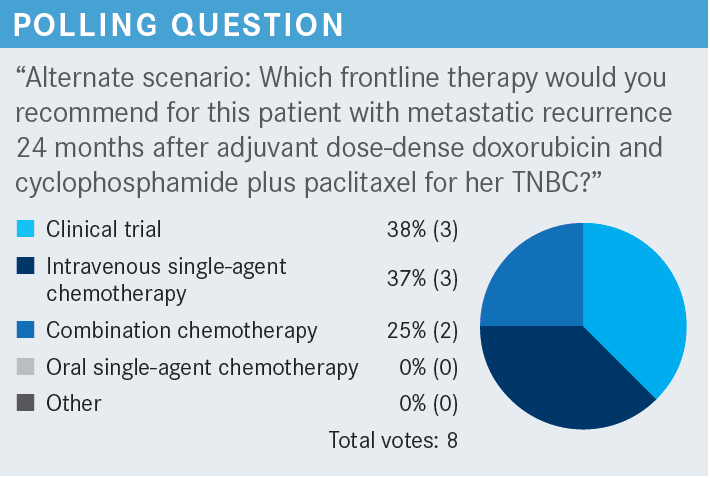
CHAUNCEY: I am thinking about repeating the taxane.
CONLIN: So, going back to a taxane because it has been 24 months. Presumably capecitabine is still an option.
BORKOWSKI: I was leaning toward clinical trial, and I always like that capecitabine is easy. It would be something to try, depending on how much she was ready to jump into combination chemotherapy.
CONLIN: That’s a good option.


CONLIN: Let’s assume her liver numbers still look fairly good, and she has a lot of healthy liver left to tolerate another line of therapy.


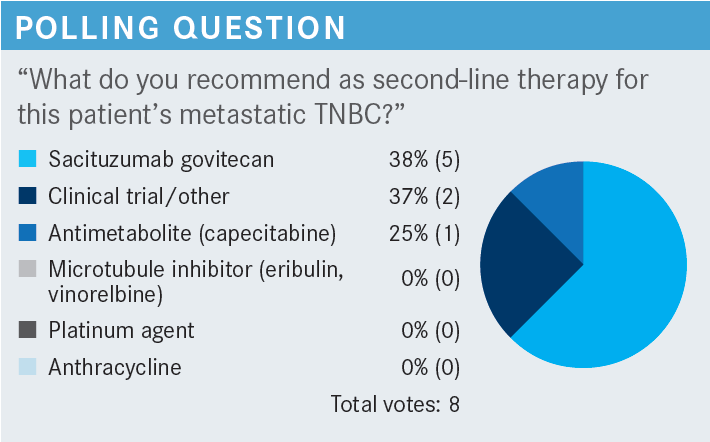
CONLIN: We are seeing that sacituzumab govitecan [Trodelvy] is showing up with 63%, so most of us are voting for that as our second-line agent. There is still a vote for the capecitabine. Clinical trial still shows up, but as we know, that’s not always available, or patients aren’t always available or able to get [into] trials.
GOLDBERG: I originally voted for clinical trials [because] she had absolutely no response to begin with. I just think with no response to effective chemotherapy, it is doubtful she would respond to the capecitabine or other options. With the clinical trial, at least we would learn something from it.
CONLIN: How about if, with second-line therapy, she does respond to some chemotherapy, and you feel like she is a little more sensitive? What would you give then?
GOLDBERG: I’d join the majority and give sacituzumab govitecan. I would give that, probably holding the clinical trial next.
CONLIN: I’m surprised we didn’t get any eribulin votes, but that’s OK.
SHENOI: I chose sacituzumab. It’s the new kid on the block, has a lot of good data, and is exactly the second line to give after progression. The data explain why we need to choose that drug, and I chose it.
CONLIN: Oncologists think the ideal sequence is a chemotherapy, then sacituzumab. If you don’t have a clinical trial, I think gemcitabine plus carboplatin seems reasonable [for first-line therapy] because the patient hasn’t had platinum therapy. Then think about sacituzumab [for second-line therapy]. I think we mentioned she didn’t have a BRCA mutation.


CHINTAPATLA: I had an experience with sacituzumab in 2 patients. Both tolerated the treatment well, with response within a few months. The only thing I would say is that if patients have liver metastasis and elevated liver function tests, they seem to have a little more toxicity in terms of the cytopenia compared with patients without liver metastasis. I don’t know [whether] that is documented.
CONLIN: Did you have to do any dose reductions in those patients?
CHINTAPATLA: Yes, I did for 1 patient due to cytopenia.
CONLIN: Does anyone ever use growth factor support with sacituzumab?
WANG: I have tried to, but it was not approved by insurance. I think the guidelines say the patient must have a neutropenic fever, but it was not approved.
CONLIN: So in that case, did you dose reduce instead?
WANG: I didn’t [at first]. My patient had a tough time. She was tolerating all the previous chemotherapy very well, but this was a tough drug for her, so she was having diarrhea and prolonged neutropenia, and I think she was hospitalized for the diarrhea. The toxicities were worse than I was prepared for.
CONLIN: It sounds like she was heavily pretreated, but yes, she also struggled with the treatment.
WANG: I eventually had to dose reduce for various reasons— mostly for fatigue and diarrhea.
YAN: My experience has been pretty good. I have treated quite a few patients with sacituzumab govitecan. I was fortunate that it was approved for 1 patient as [second]-line therapy after the KEYNOTE-522 [NCT03036488] regimen.
The other patient had TNBC heavily treated with a lot of monotherapies, and quite a few were mixed. They had a lot of alopecia, and because it’s an ADC [antibody-drug conjugate], I was not prepared for the grade 3 alopecia. For neutropenia, I had pegfilgrastim [Neulasta] approved on day 8, so it was never an issue for me. So far, I have not had to dose reduce sacituzumab.
CONLIN: So you have used a long-acting [granulocyte colony-stimulating factor] on day 8 and not had to dose reduce. Are you doing that for everybody or just depending on the patient’s [response]?
YAN: It depends on the patients. I do not get it approved up front, I wait. From my experience, for a lot of my patients, I don’t do day 8 treatment. Although day 8 neutropenia is common, I have been scheduling them at around day 10. That’s when the neutropenia can recover. I have a lot of patients tell me they must come back a day or 2 after day 8, so I tell them not to come back on day 8 but on day 10 or 11, and it has been working out for me. When they have repetitive neutropenia, I [can] get pegfilgrastim approved, so I never need to reduce the dose because of neutropenia. I dose reduce for other reasons, but not for neutropenia.
CONLIN: Have you had struggles with diarrhea, as well, or not so much?
YAN: Not so much. I did have 1 patient with TNBC who had diarrhea previously from other regimens, so when diarrhea happened, she did not even blink on this treatment. I gave her a lot of diphenoxylate/atropine [Lomotil] and she was fine. Diarrhea can happen, but we are oncologists, and I feel we can manage that.
CONLIN: I have not seen so much of the diarrhea, just like you. Maybe some of these patients are already prepared on what to use for diarrhea. Initially, I was a little surprised about nausea. I find we always assume we are not going to see nausea [with ADCs], now we know that’s not nearly the case.
I have had patients with a little neutropenia and other hematologic toxicities. I don’t think I’ve had to use as much growth factor support, but I am probably more likely to maybe hold or dose reduce, but growth factor support seems like a good option.
YAN: Yes, this is exactly why I am an advocate for using growth factor therapy earlier rather than later, because if the patient is heavily treated, adverse effects [AEs] are more common. But if they are not heavily treated, then AEs are not as common.


CHAUNCEY: In the ASCENT study, did patients stop the drug at the time of progression?
CONLIN: Yes.
CHAUNCEY: It seems like there’s a disconnect, or maybe I am not used to looking at this group of patients in a trial. But the OS [overall survival] benefit was profound, even though the PFS [progression-free survival] was less so, and it was persistent [median PFS, 5.6 months vs 1.7 months; median OS, 12.1 months vs 6.7 months].1,2
Did the patients who progressed get other treatment? Did this somehow potentiate the treatment beyond stopping the drug?
CONLIN: Those are good questions and observations. I think patients who potentially don’t respond may die quickly. I think we see this with patients. We can’t even get a next line of therapy before they end up having liver or respiratory failure. [It happens] before you get something approved. So those who aren’t responding are making that difference, potentially. It is a good question. When there is crossover, it’s not planned, and patients have access to other things, you don’t know where the survival benefit is from.
CHAUNCEY: There is a big difference in OS.


CONLIN: In our case, the patient had a biopsy when she first presented. Are you getting any special molecular testing, or doing biopsies on all patients? Will everybody share what they generally do when patients present with metastatic disease?
I try to biopsy my patients and do some molecular testing to look for TNBC and PD-L1 expression, but also any targetable mutations and their BRCA mutational status.
GOLDBERG: Overall, we are getting much more aggressive in testing now. Hopefully insurance gives us the OK, but it’s getting to be a necessity. [We send out to] FoundationOne and [Tempus].
CHINTAPATLA: We test on a routine basis—mostly [next-generation sequencing] to the Providence [St Joseph Health Molecular Genomics Laboratory].


CONLIN: [Sacituzumab] is an ADC targeted to Trop-2, and of the patients on the trial, [approximately] 80% or so had Trop-2 expression. [However], we are not sure whether that seemed to be the selection of the population that needed it. I am not sure I’ve seen that kind of testing anywhere.
Is anyone doing any trials on this or have anything they want to share on this?
YAN: No, [Trop-2 testing] does not help at all. We can test for that if we want to, but I do not feel it helps me with any decisions, so I don’t send them.
CONLIN: Right, so you aren’t sending it for your practice. Let’s say the patient gets gemcitabine plus carboplatin first because it is a short sequence, then sacituzumab. What would be the thing you might use after?
CHINTAPATLA: Capecitabine [would be] my other option.
CONLIN: It probably depends a lot on what is going on with the patient. If they are having rapidly progressive liver disease, what is safe to give them in terms of dosing? If they need a break from coming in all the time, maybe capecitabine is a nice option for when people want to not be there as much, physically sitting in the chairs.
SHENOI: If the patient was BRCA positive with metastasis, would you consider olaparib [Lynparza] plus carboplatin?
CONLIN: There are [data for] the olaparib plus carboplatin regimen, but I haven’t given them together. Olaparib is a nice option for patients. It is oral, but it does have a toxicity profile that is not completely benign, with hematologic toxicities, fatigue, and nausea, as well. But again, it depends on how sick a patient is or how quickly I feel like I need a response. But it feels like a good thing for patients, [for you] to be able to say, “I have a target on the tumor that we can address with a PARP inhibitor.” So, I might start with it sooner.


GOLDBERG: They are all important when you are getting to this point. You must put the whole patient together again, and quality of life [QOL] is No. 1, then you think about selecting something with the best chance without significant burdening of the patient. Because chances are, with third-line therapy, you are not making big home runs here. I think OS and PFS, but QOL is important, too, so you must weigh that with what you are going to try.
CONLIN: Do you worry about the patients’ age or their other comorbidities? Does that factor in for you, as well?
GOLDBERG: Performance status is in there, [as well as] frailty, which would cover all the other comorbidities and factors like that. If they have a certain comorbidity that would be, for a certain drug, detrimental going forward, [then] yes. One must then weigh QOL and toxicity of each drug, so when you go to a third-line option, you are more flexible. That’s why capecitabine is a nice drug. I almost think it’s the hospice drug. We all use it because it’s so easy, and I’m not sure whether we are doing anything [for the disease] on third-line therapy. It would be nice to have clinical trials, except clinical trials of third-line agents don’t look too good either, because patients have been [through a lot]. It’s a complex decision.
CONLIN: I agree. You are hitting on a lot of important points. For capecitabine, we all know what you mean. The other point about trials in the third-line setting is that people who have these great performance statuses on third-line therapy [might] have a special type of TNBC. Those might be a different selection of people in the real world. How easy is it to have someone who can wait 3 weeks to get the tests done, have good laboratory results, and have all the good stuff that gets you on the study? If we get those patients, we certainly want to have the data show great options for them.
WANG: I agree and disagree, because everyone is different in a way that is not just age, performance status, or QOL. That matters the most for me. I have some patients who—if you hold chemotherapy for 1 week, we have all the disease coming out and it is out of control—I absolutely cannot allow to go on vacation for a week because it will be out of control. I have another patient with metastatic TNBC who has survived for 5 years, so far. There are outliers.
I am looking at my patients and asking them and myself whether we have the luxury to wait and [whether] they have a relatively [stable] disease—or we don’t even have the luxury to wait for 1 week. So when it comes to third-line therapy and you don’t have the luxury to miss the androgen receptor [but] I have the luxury to send for genomic tests, then I can be creative. There are some patients—because it’s so aggressive as a continuous chemotherapy—who can never take any breaks. Some patients feel better with chemotherapy because the cancer is giving all the symptoms.
REFERENCES
1. Bardia A, Hurvitz SA, Tolaney SM, et al; ASCENT Clinical Trial Investigators. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384(16):1529-1541. doi:10.1056/NEJMoa2028485
2. Kalinsky K, Oliveira M, Traina TA, et al. Outcomes in patients (pts) aged ≥65 years in the phase 3 ASCENT study of sacituzumab govitecan (SG) in metastatic triple-negative breast cancer (mTNBC). J Clin Oncol. 2021;39(suppl 15):1011. doi:10.1200/JCO.2021.39.15_suppl.1011






















