Socinski Reviews Targeted Treatment in NSCLC and ES-SCLC
During a Targeted Oncology case-based roundtable event, Mark A. Socinski, MD, discussed the results of clinical trials supporting the use of targeted agents in patients with late-stage lung cancers.



Mark A. Socinski, MD
Executive Medical Director (Thoracic Cancer)
AdventHealth Cancer Institute
Orlando, FL
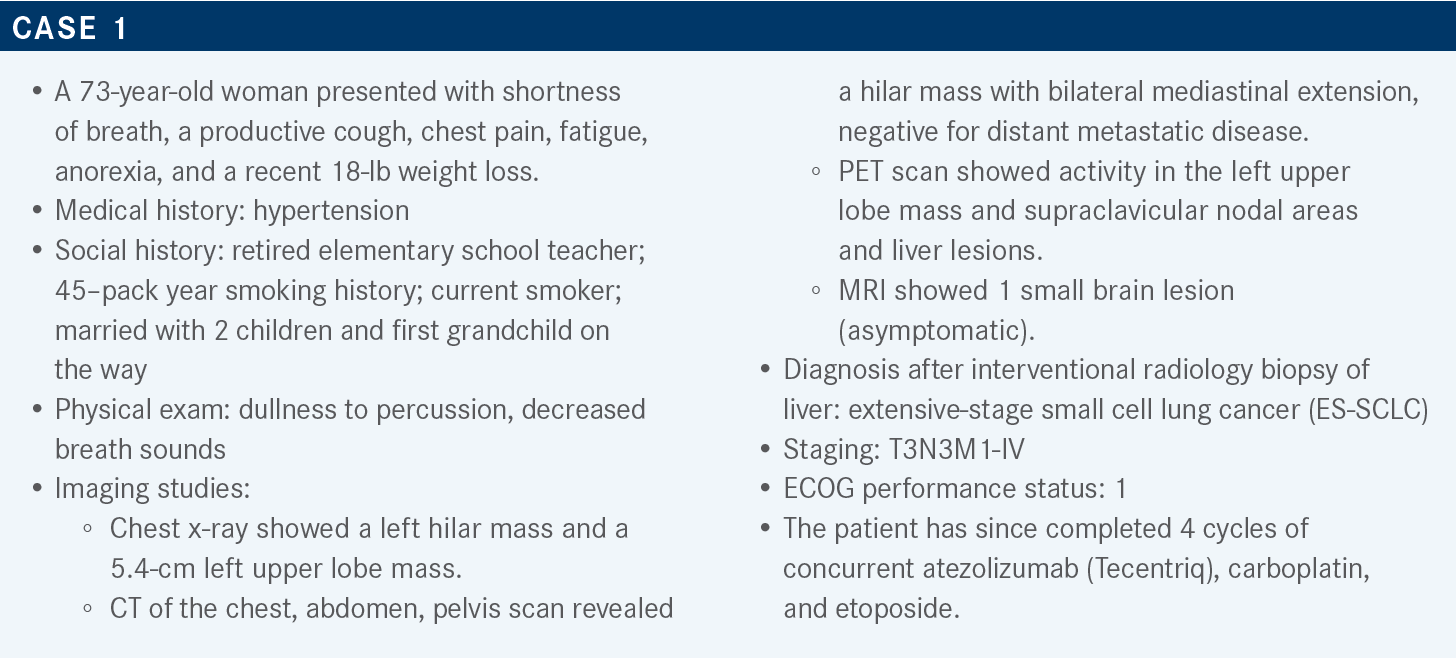
Targeted OncologyTM: What data support the addition of atezolizumab to a regimen of platinum-based chemotherapy and etoposide for patients with ES-SCLC?
SOCINSKI: The phase 3 IMpower133 trial [(NCT02763579) used this regimen to treat patients with] ES-SCLC. The patients had a good performance status and were treatment naive, and patients with asymptomatic brain metastases were eligible. [Investigators stratified] patients according to sex, performance status [0 or 1], and the presence or absence of brain metastases. Patients received the very standard 4 cycles of carboplatin and etoposide, plus either atezolizumab or placebo.
After 4 cycles of this regimen, patients received maintenance therapy with either atezolizumab or placebo. Treatment continued until disease progression or loss of clinical benefit. The primary end points were survival and investigator-assessed progression-free survival [PFS].1 PFS favored atezolizumab vs placebo with an HR of 0.77 [95% CI, 0.62-0.96; P = .02]. The absolute difference at 1 year was about a 2.5-fold increase in the percentage of patients free of progression [12.6% vs 5.4%, respectively]. The median PFS values were about the same, 5.2 months [95% CI, 4.4-5.6] and 4.3 months [95% CI, 4.2-4.5], respectively. The survival curves come together at a couple of different points in this setting.1
The overall survival [OS] data for the 2 groups revealed a difference of about 2 months [12.3 months (95% CI, 10.8-5.8) vs 10.3 months (95% CI, 9.3-11.3), respectively; HR, 0.76; P = .0154]. The data at 1 year showed about a 13 [percentage-point] OS increase in the atezolizumab group relative to the placebo group [51.9% vs 39.0%, respectively], and the relative benefit was about the same at 18 months. The curves got a little unstable after that.2
OS was also examined according to prespecified subgroups; at that time the median follow-up was about 2 years. The data suggest that atezolizumab was favored in all the subgroups except [perhaps] the subgroup of patients with brain metastases, a group of only 35 patients. Interestingly, blood tumor mutational burden was not a predictive marker for benefit of immunotherapy [IO] in this setting.2 Objective response rates [ORRs] in both groups were around 60%. Also in both groups, about 20% of patients had stable disease as their best response, and about 7% to 10% had progressive disease as their best response.1
That is pretty standard for ES-SCLC. There were no surprises in the adverse event [AE] data. I think the toxicity of carboplatin plus etoposide is well known, so I won’t focus on the placebo group. The data for the atezolizumab group are not dramatically different. My conclusion, given the vast number of trials in SCLC and in non-SCLC [NSCLC], is that if you combine IO and chemotherapy, you don’t change the toxicity profile of either the IO or the chemotherapy. [However], because you’re using more drugs, you’ll see more toxicity, as we would expect. Most of [the toxicity consists of] immune-related AEs.1
Which trial demonstrated the efficacy of durvalumab [Imfinzi] vs a platinum agent plus etoposide for patients with ES-SCLC?
In the CASPIAN trial [NCT03043872], the control arm was a platinum agent [carboplatin or cisplatin] plus etoposide, and this was compared with durvalumab plus the control combination. As in IMpower133, the population consisted of treatment-naive patients. Maintenance was given as expected in this setting [durvalumab for the experimental arm; platinum agent plus etoposide for the control arm, with an option for prophylactic cranial irradiation]. The primary end point was OS and the secondary end points included PFS, ORR, and safety.3
After a median follow-up of over 3 years, the HR for 3-year OS with the addition of durvalumab was 0.71 [95% CI, 0.60- 0.86; P = .0003]. At 2 years, there was about a 9 [percentage point] difference in the probability of OS, and that [persisted] at 3 years, with about 6% of patients alive on the control arm and about 18% alive on the durvalumab arm.4
Analysis of 3-year OS in the preplanned subgroups revealed that the experimental regimen was favored in all subgroups, including the subgroup of patients with brain metastases. The number of patients in that subgroup was relatively small [as in IMpower133], and there was a very wide confidence interval, but this [result] was certainly consistent with [those of all] the other subgroups in terms of benefit.4 Analysis of PFS revealed an HR of 0.80 [95% CI, 0.66-0.96]. At 1 year and at 2 years, the percentage of patients free of progression was about 3-fold greater in the experimental group relative to the control group.5
The ORR was a bit better for the durvalumab arm than for the control arm [68% vs 58%, respectively; odds ratio, 1.53; 95% CI, 1.08-2.18] and, as with many IO trials, the duration of those responses was significantly better in patients who received durvalumab.6 The results of this trial were similar to those of IMpower133 in terms of toxicity. Between the control group and the durvalumab group, there were very similar rates for all-grade, all-cause AEs and for grade 3 and grade 4 AEs. This trial included another arm, which we did not discuss here. Patients in that third arm received tremelimumab in addition to durvalumab, etoposide, and a platinum agent. As expected, there was more toxicity with the dual IO therapy.6
How do the IMpower133 and CASPIAN trials compare?
Between-trial comparison revealed similar median OS values on the investigational arms [12.3 months and 12.9 months for the experimental arms of the respective trials] and on the control arms [10.3 months and 10.5 months, respectively], with similar HRs [0.76 (95% CI, 0.60-0.95) and 0.71 (95% CI, 0.60- 0.86), respectively].
The PFS numbers were also similar [5.2 months and 5.1 months for the respective experimental arms; 4.3 months and 5.4 months for the respective control arms], again with similar HRs [0.77 (95% CI, 0.62-0.92) and 0.80 (95% CI, 0.66- 0.96), respectively]. Relative to the ORRs of both arms of the IMpower133 trial [60.2% for the experimental arm and 64.4% for the control arm], the ORR of the CASPIAN durvalumab arm was slightly higher [67.9%] and the ORR of the CASPIAN control arm was slightly lower [58.06%].
The rates of AEs of grade 3 or greater were very similar between the trials [67.7% and 62.3% for the respective experimental arms; 63.3% and 62.8% for the respective control arms]. Immune-related AEs were certainly higher in IMpower133 than in CASPIAN [41.4% and 20.0% for the respective experimental arms; 24.5% and 2.6% for the respective control arms].1-7 That may be more of a recording issue; I don’t get the sense that atezolizumab and durvalumab are dramatically different in that regard.
What are some practical considerations when using these regimens?
You do have some flexibility [when choosing a] platinum partner to use with durvalumab. Dosing and administration are particularly pertinent for the maintenance phase, when you can make [the therapy] a little more convenient. The warnings and precautions are fairly similar between the 2 regimens.8,9

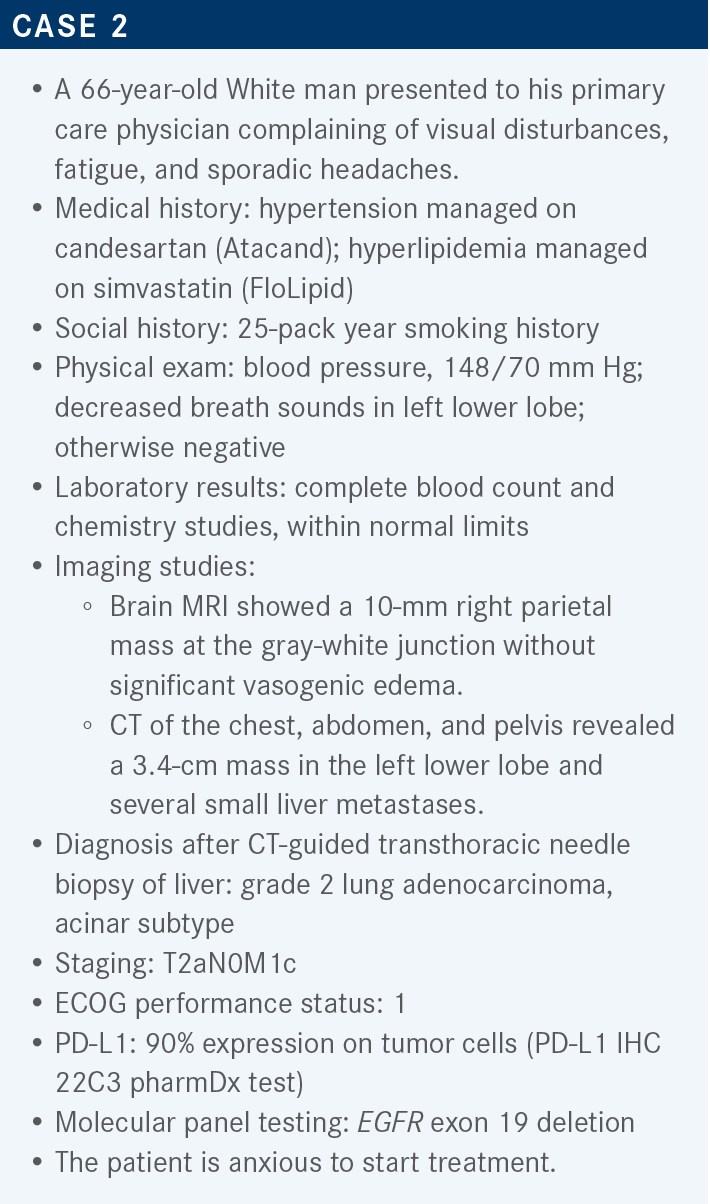
What should a physician consider when choosing and sequencing therapies if PD-L1 expression is positive and EGFR is mutated?
SOCINSKI: In a case like this one, if you act on the 90% PD-L1 positivity, and you use a PD-1/PD-L1 inhibitor, it can set the patient up for a risk of increased toxicity with osimertinib [Tagrisso]. Certainly pembrolizumab [Keytruda], even in high expressors, is just not effective in this population.10-12 PD-L1 [positivity] has a different meaning if you have an oncogenic driver. What’s driving the disease is not the immune system; what’s driving the disease is the kinase activity that’s being turned on by the mutation or fusion that you’ve detected, so IO is just not effective therapy. Targeted therapy is the way to go.
For nonsquamous advanced NSCLC with at least 1 actionable mutation, the Society for Immunotherapy of Cancer recommends targeted therapy [first, followed by] chemotherapy, and then, as a last resort, checkpoint inhibitors as third-line therapy.13
What data have illustrated the risk of treating patients like this one with PD-1/PD-L1 blockade followed by osimertinib?
In one study [NCT02879994], researchers treated PD-L1–positive, EGFR mutation–positive, advanced NSCLC with pembrolizumab. They stopped enrollment after the first 11 patients [because of absence of efficacy]. Among these patients, 73% had PD-L1 expression greater than 50%. Only 1 patient had an OR, and that patient was later found actually to be EGFR-mutation negative. Because [the patients] didn’t respond, they were treated with EGFR tyrosine kinase inhibitors [TKIs], specifically osimertinib, and there were 2 deaths within 6 months of enrollment, including 1 attributed to pneumonitis.10
If you make the wrong decision by not waiting, you can cause a problem for the patient. You may not kill them, but they might have an adverse reaction that prevents them from [receiving] osimertinib, which is actually their best treatment. So the take-home message is that this sequence can be dangerous and that you need to wait. Now obviously, there are some patients you feel you have to treat. [In that case], just give a cycle of chemotherapy. It buys you 3 weeks and you’re very likely to get some clinical benefit with the first cycle of chemotherapy. This seems to be an issue principally with osimertinib. This has not been seen either with erlotinib [Tarceva] or with the [reverse] sequence—giving an EGFR-targeted TKI first followed by PD-1/ PD-L1 blockade.11
In an analysis of severe immune-related AEs experienced by patients who received osimertinib after PD-1/PD-L1 blockade, [the most common was] pneumonitis. Many of the patients were hospitalized because of the toxicity, so this is serious stuff, and it would preclude them from getting osimertinib [again, which would otherwise be] their best treatment option.11
Have any studies compared the effectiveness of PD-1/PD-L1 inhibitors with that of docetaxel as second-line therapy in patients with and without EGFR mutations?
A meta-analysis examined 5 trials and 3000 patients; EGFR status was available for most of the patients. The EGFR-mutated patients did not experience OS benefit from a PD-1/PD-L1 inhibitor vs docetaxel; actually, there was a trend toward a benefit from docetaxel. In contrast, the population with wild-type EGFR got a significant benefit from PD-1/PD-L1 inhibitors vs docetaxel. This is another example showing that checkpoint inhibitors don’t have a great deal of activity in the setting of these driver mutations or fusions.14

What data support the use of osimertinib as a first-line therapy for NSCLC in a patient like this one?
The FLAURA trial [NCT02296125] examined the use of osimertinib in this setting. Patients in this trial were treatment-naive and had a good performance status. They had EGFR mutations in exon 19 or 21, and patients with stable brain metastases were allowed to participate. Patients in the comparator arm received either of the first-generation drugs erlotinib or gefitinib [Iressa]; patients in the experimental arm received the third-generation drug osimertinib. Treatment continued until progression or unacceptable toxicity. The primary end point was PFS; secondary end points included ORR, OS, duration of response, and safety.15
I love clinical trials [like this one for which] you don’t need a statistician to tell you which [regimen] is better. In this case, you have almost a doubling of the median PFS in the experimental arm relative to the comparator arm [18.9 months vs 10.2 months, respectively; HR, 0.46; 95% CI, 0.37-0.57; P < .0001].15
Interestingly, I’m not sure I would have bet on there being an OS benefit with osimertinib vs the first-generation drugs, but there was a benefit [for median OS at 38.6 months vs 27.0 months, respectively; HR 0.799; 95% CI, 0.641-0.997; P = .0462].16 Remember, our job as oncologists is to get the right treatment to the right patient at the right time. It’s got to be the best treatment, and these are very convincing data with regard to OS.
REFERENCES
1. Horn L, Mansfield AS, Szczęsna A, et al; IMpower133 Study Group. First-Line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220-2229. doi:10.1056/NEJMoa1809064
2. Liu SV, Reck M, Mansfield AS, et al. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J Clin Oncol. 2021;39(6):619- 630. doi:10.1200/JCO.20.01055
3. Paz-Ares L, Dvorkin M, Chen Y, et al; CASPIAN Investigators. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929-1939. doi:10.1016/ S0140-6736(19)32222-6
4. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab ± tremelimumab + platinum-etoposide in first-line extensive-stage SCLC (ES-SCLC): 3-year overall survival update from the phase III CASPIAN study. Ann Oncol. 2021;32(suppl 5):S1283- S1346. doi:10.1016/annonc/annonc741
5. Goldman JW, Dvorkin M, Chen Y, et al; CASPIAN Investigators. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2021;22(1):51-65. doi:10.1016/S1470-2045(20)30539-8
6. Paz-Ares LG, Dvorkin M, Chen Y, et al. Durvalumab ± tremelimumab + platinum-etoposide in first-line extensive-stage SCLC (ES-SCLC): updated results from the phase III CASPIAN study. J Clin Oncol. 2020;38(suppl 15):9002. doi:10.1200/ JCO.2020.38.15_suppl.9002
7. Reck M, Liu SV, Mansfield AS, et al. IMpower133: updated overall survival (OS) analysis of first-line (1L) atezolizumab (atezo) + carboplatin + etoposide in extensive-stage SCLC (ES-SCLC). Ann Oncol. 2019;30(suppl 5):V710-V711. doi:10.1093/annonc/mdz264
8. Tecentriq. Prescribing information. Genentech Inc; 2022. Accessed April 7, 2022. https://bit.ly/3s0Yku5
9. Imfinzi. Prescribing information. AstraZeneca Pharmaceuticals LP; 2021. Accessed April 7, 2022. https://bit.ly/36XsaIt
10. Lisberg A, Cummings A, Goldman JW, et al. A phase II study of pembrolizumab in EGFR-mutant, PD-L1+, tyrosine kinase inhibitor naïve patients with advanced NSCLC. J Thorac Oncol. 2018;13(8):1138-1145. doi:10.1016/j. jtho.2018.03.035
11. Schoenfeld AJ, Arbour KC, Rizvi H, et al. Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib. Ann Oncol. 2019;30(5):839-844. doi:10.1093/annonc/mdz077
12. NCCN. Clinical Practice Guidelines in Oncology. Non-small cell lung cancer, version 3.2022. Accessed April 7, 2022. https://bit.ly/3vpqVLs
13. Brahmer JR, Govindan R, Anders RA, et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of non-small cell lung cancer (NSCLC). J Immunother Cancer. 2018;6(1):75. doi:10.1186/ s40425-018-0382-2
14. Lee CK, Man J, Lord S, et al. Clinical and molecular characteristics associated with survival among patients treated with checkpoint inhibitors for advanced non-small cell lung carcinoma: a systematic review and meta-analysis. JAMA Oncol. 2018;4(2):210-216. doi:10.1001/jamaoncol.2017.4427
15. Soria JC, Ohe Y, Vansteenkiste J, et al; FLAURA Investigators. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113-125. doi:10.1056/NEJMoa1713137
16. Ramalingam SS, Vansteenkiste J, Planchard D, et al; FLAURA Investigators. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41-50. doi:10.1056/NEJMoa1913662