Quinn Explores Treating Metastatic CRPC in Men With Germline or Somatic Mutations
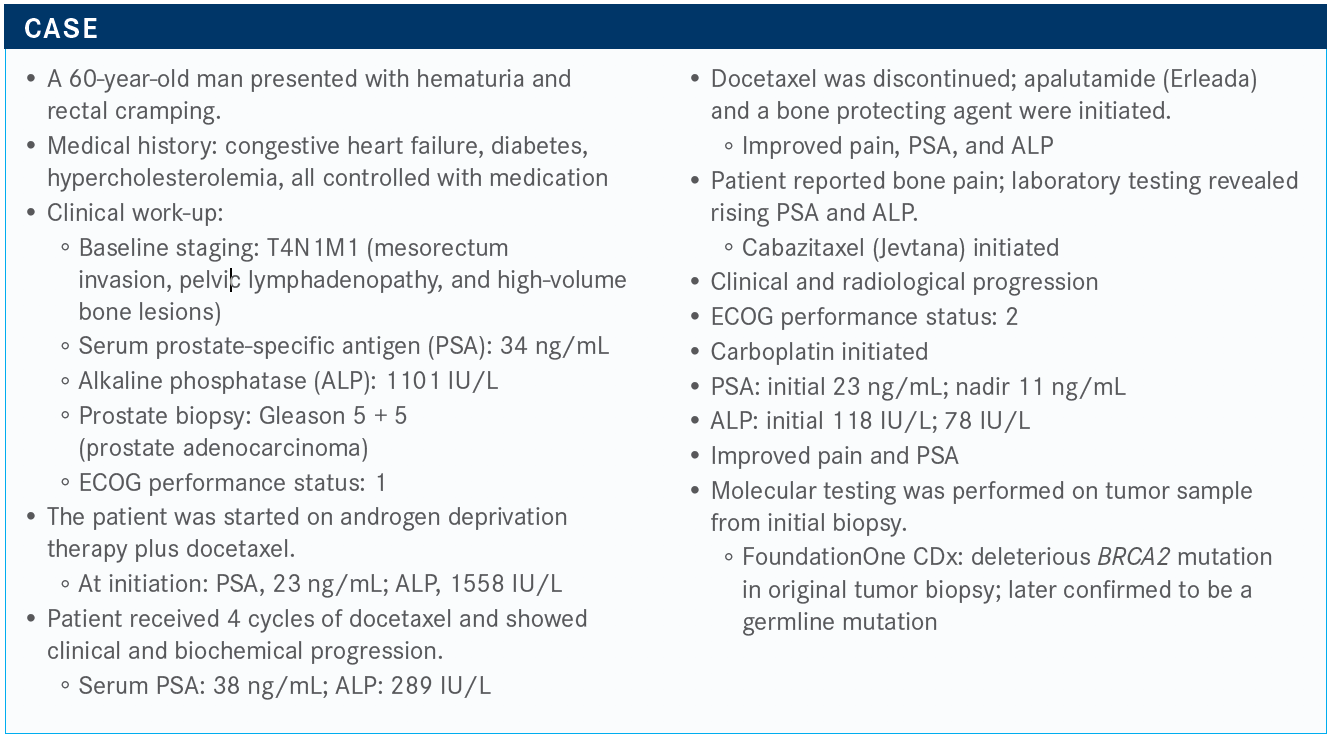
During a virtual Case Based Peer Perspectives event, David I. Quinn, MD, MBBS, PhD, reviewed the case of a 60-year old male patient with metastatic castration-resistant prostate cancer.


David I. Quinn, MD, MBBS, PhD
During a virtual Case Based Peer Perspectives event, David I. Quinn, MD, MBBS, PhD, associate professor of Medicine, Section Head, Genitourinary Oncology, Division of Cancer Medicine and Blood Diseases, Department of Medicine, University of Southern California, Los Angeles, CA, reviewed the case of a 60-year old male patient with metastatic castration-resistant prostate cancer. He also discussed the treatment options for patients harboring either a germline or somatic mutation.


Targeted Oncology™: How is the patient's BRCA2 mutation significant and what data support that?
QUINN: There were 2 TRITON studies. TRITON2 [NCT02952534] is a phase 2 study and TRITON3 is a phase 3 study [NCT02975934]. TRITON3 has just closed. TRITON2 led to the accelerated approval of rucaparib [Rubraca].
To be eligible for TRITON2, patients had to have metastatic castration-resistant prostate cancer [mCRPC].1 Patients received rucaparib twice daily at 600 mg. Treatment continued until radiological progression or discontinuation because of toxicity, death, or illness from other cause. The primary end point was response in patients with measurable disease at baseline and confirmed by PSA response [of ≥50% PSA for patients with nonmeasurable disease].
The study enrolled 85 patients, and the investigators evaluated the populations with PSA response. Forty-five patients had BRCA1 or BRCA2 mutations. There were 18 patients with ATM alterations, 13 with CDK12, and...a hodgepodge of others who were also evaluated. And that was the PSA response evaluable populations. They had to have PSA present to a certain level to qualify, so most of them qualified but not all. Patients with measurable disease and [more than] 16 weeks of follow-up were reviewed using RECIST. That is why when we’re looking at the responses, we have presentation of PSA response and presentation of RECIST response.
What was the response rate for patients on this trial?
For patients with measurable disease, the response rate was 44%, 11 of 25. It was mainly responses in BRCA1/2, although there were responses in a patient with a BRIP1 and a patient with a FANCA alteration [TABLE on page 11].1
In patients with ATM and CDK12 alterations, the best response was stable disease. I followed a number of people with ATM1 who were taking PARP [inhibitors], and they often have stable disease. But it can remain stable for a long time with a PSA that is also stable. Many patients had durable responses to rucaparib.
These data contributed to the subsequent accelerated approval by the FDA for rucaparib in patients with BRCA1/2 mutations.
Looking at PSA responses, half of the patients with BRCA1/2 had a PSA response. The best change for PSA was observed in BRCA1/2.
What should we keep in mind for patients who don’t have BRCA1/2?
In patients who don’t carry BRCA1/2, we observe a 6-month clinical benefit of about 28% in patients with ATM. It is observed with CDK12 and also in CHEK2. You just need to be aware that there are other markers that signal a change, other than a change in PSA.
What are the adverse effects associated with PARP inhibitors?
We have several PARP inhibitors available to us, and they all have adverse eff ects across the board. The most common are asthenia, nausea, anemia, liver enzyme changes, and peripheral edema. Most of these are not grade 2 or 3, but they can become cumulative over time, especially after 6 months.
Do we have evidence of the benefit of olaparib (Lynparza) in either the somatic or germline alteration setting?
The PROfound study [NCT02987543] evaluated olaparib as a treatment for patients with somatic or germline alterations.2,3 Patients were stratifi ed into 2 groups. Group 1 consisted of patients with BRCA1/2 or ATM, and group 2 included patients with other alterations.
Patients were randomized to receive either olaparib 300 mg twice a day or physician’s choice of therapy. The study end point was radiographic progression-free survival [PFS], and there was also a secondary end point of confirmed radiographic objective response rate.
The investigators found at least 1 alteration in prespecified homologous recombination repair [HRR]–associated genes in 28% of 2792 samples.
If we look at the primary outcome for PROfound, there is a major advantage in PFS for the PARP inhibitor at 7.4 months compared with physician’s choice at 3.6 months [HR, 0.34; 95% CI, 0.25-0.47; P < .001]. If both cohorts are combined, we still see a favorable benefit for olaparib at 5.8 months versus 3.5 months for the control arm [HR, 0.49; 95% CI, 0.38-0.63; P < .001].
Looking at PFS by subgroup, olaparib is still favored over the control group. ATM equally responds to both, and CDK shows no advantage toward either treatment. You don’t get a response just because of the presence of an alteration.
The interim analysis of overall survival for cohort A showed a benefit for olaparib at 17.5 months versus 14.3 months for the control group [HR, 0.67; 95% CI, 0.49-0.93; P = .00630].3 For time to pain progression, patients in the olaparib group had a 33% confirmed objective response rate versus 2% for the control [OR, 20.86; 95% CI, 4.18-379.18; P <.001]. So it was quite delayed for patients in the olaparib arm. PARP inhibitors are palliative as well as therapeutic in terms of producing a response in PSA and RECIST criteria.
References
1. Abida W, Bryce AH, Vogelzang NJ, et al. Preliminary results from TRITON2: a phase 2 study of rucaparib in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) associated with homologous recombination repair (HRR) gene alterations. Ann Oncol. 2018;29(suppl 8; abstr 3619):viii271-viii302. doi:10.1093/annonc/mdy284
2. Hussain M, Mateo J, Fizazi K, et al. PROfound: phase 3 study of olaparib versus enzalutamide or abiraterone for metastatic castration-resistant prostate cancer (mCRPC) with homologous recombination repair (HRR) gene alterations. Ann Oncol. 2019;30(suppl 5; abstr 5059):v851-v934. doi:10.1093/annonc/mdz394
3. de Bono J, Mateo J, Fizazi K, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2020;382(22):2091-2102. doi:10.1056/NEJMoa1911440

















Survivorship Care Promotes Evidence-Based Approaches for Quality of Life and Beyond
March 21st 2025Frank J. Penedo, PhD, explains the challenges of survivorship care for patients with cancer and how he implements programs to support patients’ emotional, physical, and practical needs.
Read More




