Roundtable Discussion: Tykodi Looks at Multiple Regimens for Managing Renal Cell Carcinoma
During a Targeted Oncology case-based roundtable event, Scott Tykodi, MD, PhD, discussed the data supporting various treatment options for renal cell carcinoma with participants.




Associate Professor, Clinical Research Division
Fred Hutchinson Cancer Research Center
Associate Professor, Division of Medical Oncology
University of Washington School of Medicine")
Scott Tykodi, MD, PhD (moderator)
Associate Professor, Clinical Research Division
Fred Hutchinson Cancer Research Center
Associate Professor, Division of Medical Oncology
University of Washington School of Medicine



AHED: I like to do positron emission tomography [PET] scans; some of them will light up like Christmas trees and then some others don’t light up at all. It’s good to know [that information] from the get-go.
TYKODI: Do you find that you [have] trouble with insurance providers declining PET scans for kidney cancers?
FAHED: It depends on which plan [the patient has]. I have, in general, a lot of denials, and I have to go and appeal. That’s kind of routine.
TYKODI: What about the findings? Obviously, if you had bony lesions that you hadn’t seen on body imaging, that would probably influence at least applying bone-directed therapy.
But is there anything about the PET imaging, the intensity uptake or finding a couple of spots you didn’t see on CT imaging, that might influence…your choice of therapy?
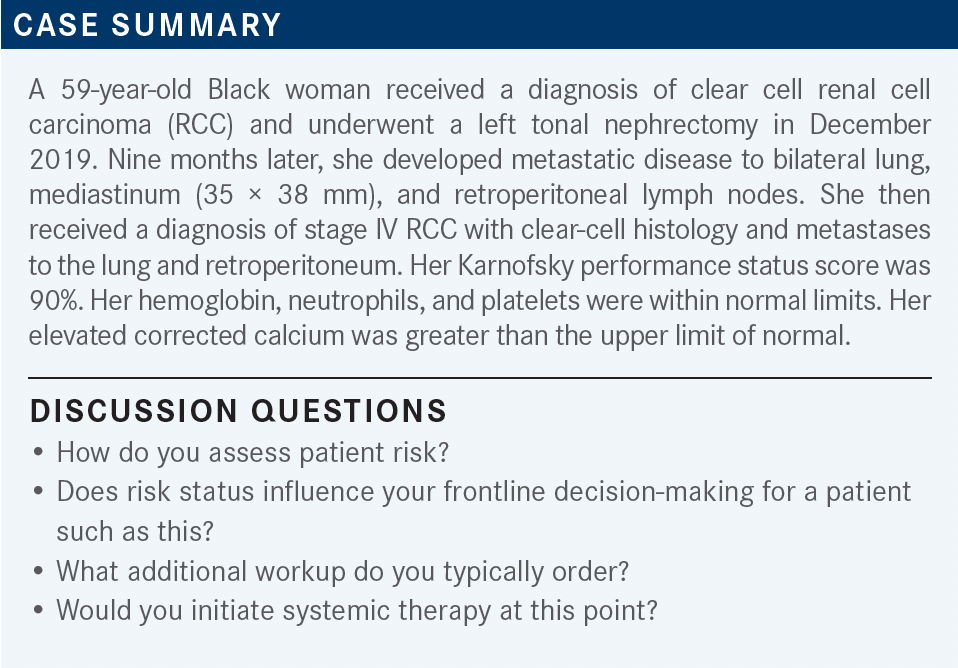
FAHED: For this patient, this is a first recurrence, and what we saw on CT imaging were some deposits in the left upper quadrant, so it wasn’t a clear-cut recurrence. Unfortunately, it did not help much in this situation.
TYKODI: For most patients with kidney cancer, would you try to get a baseline PET scan? Is that how you like to manage [this situation]?
FAHED: I see that it helps with my [patients with] bone metastases. The CT scan is not the best test to see bone metastases. A PET scan, a lot of times, does not show any bone lesions, but then you do a PET scan and you see plenty of metastatic disease.
CHINTAPATLA: For me, this patient has hypercalcemia, [so I would] initiate a bone scan. Typically, I don’t do CT scans in the kidney setting.
ZHANG: I don’t typically do a PET scan, either. On some occasions, if we want to confirm oligometastatic disease, I may do it, but I generally would do a brain MRI. I do get a brain MRI for every patient. I think…that will be in line with European recommendations to get a brain MRI.1
TYKODI: You’re saying you do it on everyone? It’s not guided by your sense of the patient’s risk…or negative histological results?
ZHANG: I think…that high-risk patients—for example, a patient with lung metastases and mediastinal lymphadenopathies—those are more likely to have brain metastases and there are some retrospective data on that, but occasionally we see surprises. Even for the patient with very good systemic control, they may have brain recurrence. I got burned a couple of times, so I started to do it more often.
TYKODI: I think the intent [in this case] was that [the patient] has new metastatic findings at 9 months from their nephrectomy, so you’re at less than a year and you’re falling within that time interval that would be a risk factor. But yes, you’re right, that is a little bit confusing.
I think that risk factors most commonly divide the population between local RCC that relapses later and synch-ronous metastatic disease, where you start treating [right at the time of diagnosis]. That’s the typical distinction. There’s always the odd patient that you follow, maybe [one who has] small lung nodules for a while, and they [survive beyond] a year.
Any other comments on work-up? Does anybody feel strongly about gene panel testing? Do you incorporate that into your practice, and if you do, what sorts of findings are [affecting] your choice of therapy?
FAHED: Before I didn’t, but I’m starting to think about it.
TYKODI: I think The Cancer Genome Atlas [states] VHL mutations are the most common or some of the most common, but you can have chromosome deletions where you lose an allele as well, that wouldn’t show up on your [next-generation sequencing] panel.
But then the question is: How does that influence your therapy, if you know they [have] a clear cell histology? Are there certain genes? Are you looking for mTOR pathway genes, or is there anything about the panel that would sway you in terms of how you choose your initial therapy?
FAHED: No, no preferential therapy for me.


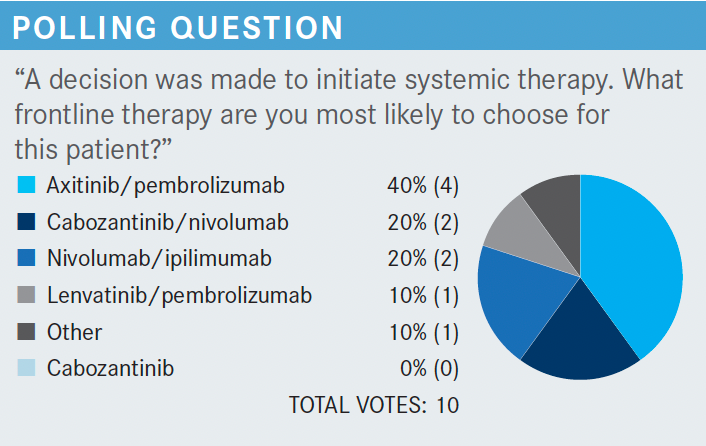
TYKODI: [When I look at the data from the CLEAR trial (NCT02811861)], what stands out to me] is the high bar in the efficacy data, the high response rate, the provocative progression-free survival [PFS], and the high complete response [CR] rate.2 How are you going to integrate pembrolizumab [Keytruda] and lenvatinib [Lenvima] into your practice, and are the data for efficacy a game-changer [to you all]?
CHINTAPATLA: I think in terms of the adverse effects [AEs] with lenvatinib [I would] not use that in [treating patients with] kidney cancer at this time.
TYKODI: How do you manage [the treatment] and adjust your practice [after] considering the CLEAR data?
QURESHI: I want to see some maturity of the data, but I [voted for] ipilimumab [Yervoy] and nivolumab [Opdivo], but I like pembrolizumab and axitinib [Inlyta] as well, especially if there are any brain metastases.
CHAVES: I think it’s a good option for first-line treatment. I’ve been more on board with axitinib and pembrolizumab previously, and I’ll have to look at the AE data [to compare] it with that, but I think it’s a good option.
CUI: I haven’t used this combination, but I use them individually for other cancers. The hypertension [that can result from taking] lenvatinib, probably to me, is more pronounced than diarrhea. I don’t know if the combination of those 2 drugs makes diarrhea worse, but the efficacy seems to be appealing.
ZHANG: I think the response rate and the CR rate are very impressive, but you know that those are used in this regimen. Lenvatinib, [when the dose is] 20 mg a day is high, and I’m concerned about the tolerability. I would consider a patient with a very high tumor burden, if I need a faster response.
TYKODI: What about lenvatinib in general? Have you used it with everolimus [Afinitor] in the salvage setting, and do you find it any more or less challenging to work with than any of the other TKIs [tyrosine kinase inhibitors] that you commonly use?
WALLEN: I haven’t used it for [patients with] RCC. I’ve used it for hepatomas on a rare occasion, but I agree with the others, that the tolerability is probably my biggest concern. The nice feature with axitinib is it’s very titratable and you can dial it up or down fairly easily.
WONG: I had a patient on lenvatinib and everolimus, and he was in kind of poor shape, but he couldn’t tolerate the lenvatinib, so we had to just take it off eventually and keep him on everolimus.
CUI: [For one patient I had,] the combination was hard. Both of those were reduced because of hypertension, even fluid overload. It’s a pretty harsh regimen.


TYKODI: To remind you all, the lenvatinib and pembrolizumab regimen starts with lenvatinib at 20 mg in combination with pembrolizumab. The everolimus and lenvatinib combination that’s currently approved as salvage therapy starts lenvatinib at 18 mg. You’re starting higher than the current use in the everolimus regimen.
So are you inclined to just dive in at 20 mg? Are you inclined to dose reduce, and what are you doing with lenvatinib and everolimus? Do you always start patients at 18 mg? Do you find that to be challenging?
ZHANG: I think I would start with 18 mg because if a patient cannot tolerate it then you may lose a patient. They lose interest in continuing. I think I would start at 18 mg instead of 20 mg, and you can always go up if they do well.
TYKODI: In the CLEAR study—and in many of the frontline studies—the immunotherapy [IO] duration is capped at 2 years, but the TKI is allowed to continue. Have you had patients get to a full 2 years of therapy, and then what are you doing for those patients?
Are you continuing a TKI? Are you continuing the IO/TKI and not being completely faithful to how the study was done? What are your thoughts about transitioning at 2 years?
QURESHI: It depends on the patient, but you know, I had a patient who still has autoimmune hepatitis as a result of her IO, so she went off. But she has remained disease-free for 2 and a half years now.
WEINER: I think if they’re doing fine and they’re not having any problems, I would be hesitant to stop things.
WALLEN: I think after 2 years, if they had a good response, I would probably start thinking about tapering the IO portion, not necessarily giving it every 3 weeks or every 4 weeks but giving it less frequently—maybe every 12 weeks or so—but continuing the TKI.
TYKODI: Has anyone had an insurance provider terminate the coverage at 2 years saying that that’s the maximum allowable duration?
INKLAB: Yes, that’s always the problem, and it depends on the diagnosis, but most of the time, for lung cancer, you will have to stop at 2 years if you have stable disease or no evidence of disease. However, if most of your patients are on Medicare, it’s not as much of an issue.


ZHANG: I think after 2 years, if they had a good response, I would probably start thinking about tapering the IO portion, not necessarily giving it every 3 weeks or every 4 weeks but giving it less frequently—maybe every 12 weeks or so—but continuing the TKI.
ANAND: I’ve used this regimen recently in a patient who had a very large tumor and metastatic disease, and she had an excellent response within 3 months and symptomatically, even after the first 2 treatments, she improved. I like this regimen, it’s very well tolerated, and her performance status improved significantly.
WALLEN: I like this regimen as well…for patients who have low tumor burden or relatively limited pulmonary metastases. I like ipilimumab and nivolumab in the first line because I think you don’t necessarily need to have a rapid response, but for [patients who] need a more rapid response, I like the IO/TKI.
This is probably 1 of my 2 favorites. The axitinib is great, too, just because it’s so eminently titratable. I think they’re comparable if you’re able to titrate the drugs up to maximum tolerable dosage.
WONG: Compared with the CLEAR trial, where [more than] 50% of patients stopped at least 1 of the drugs, in this trial it’s only 15%?
TYKODI: In CLEAR, yes, you have nearly 20% of patients stopping 1 of the 2 drugs. You should be able to add those together for stopping, because it’s the opposing drug, and then, another 10% dropping the entire regimen. Fifty percent of patients are either reducing therapy to a single drug or stopping entirely, and it’s quite different. It’s a third of that in CheckMate 9ER [NCT03141177].3
I’m curious about the practitioners who are in smaller communities, [such as] Montana and Idaho and Wyoming. Do you feel that toxicity management in patients who might geographically be more dispersed than [those] in an urban environment such as Seattle, is that more of a concern, more of an issue? Would you shy away from a regimen that you’re fearful is going to make [patients] quite ill? Do you think there’s a difference?
WEINER: I do shy away from it if a [patient] has a long travel time to get in, has difficulty coming in. I do shy away from it, but I probably go more by their performance status than anything.
QURESHI: Yes, my patient population lives close to the clinic, so I don’t have too much of an issue, but if someone’s coming from far away, I will think about that, but it doesn’t usually influence my treatment decision too much.
REFERENCES
1. Motzer RJ, Jonasch E, Agarwal N, et al. Kidney cancer, version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20(1):71- 90. doi:10.6004/jnccn.2022.0001
2. Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384(14):1289-1300. doi:10.1056/NEJMoa2035716
3. Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021;384(9):829-841. doi:10.1056/NEJMoa2026982














Enhancing Precision in Immunotherapy: CD8 PET-Avidity in RCC
March 1st 2024In this episode of Emerging Experts, Peter Zang, MD, highlights research on baseline CD8 lymph node avidity with 89-Zr-crefmirlimab for the treatment of patients with metastatic renal cell carcinoma and response to immunotherapy.
Listen


Beyond the First-Line: Economides on Advancing Therapies in RCC
February 1st 2024In our 4th episode of Emerging Experts, Minas P. Economides, MD, unveils the challenges and opportunities for renal cell carcinoma treatment, focusing on the lack of therapies available in the second-line setting.
Listen

