Randall Discusses Therapies in HRD and BRCA-Mutated Ovarian Cancer
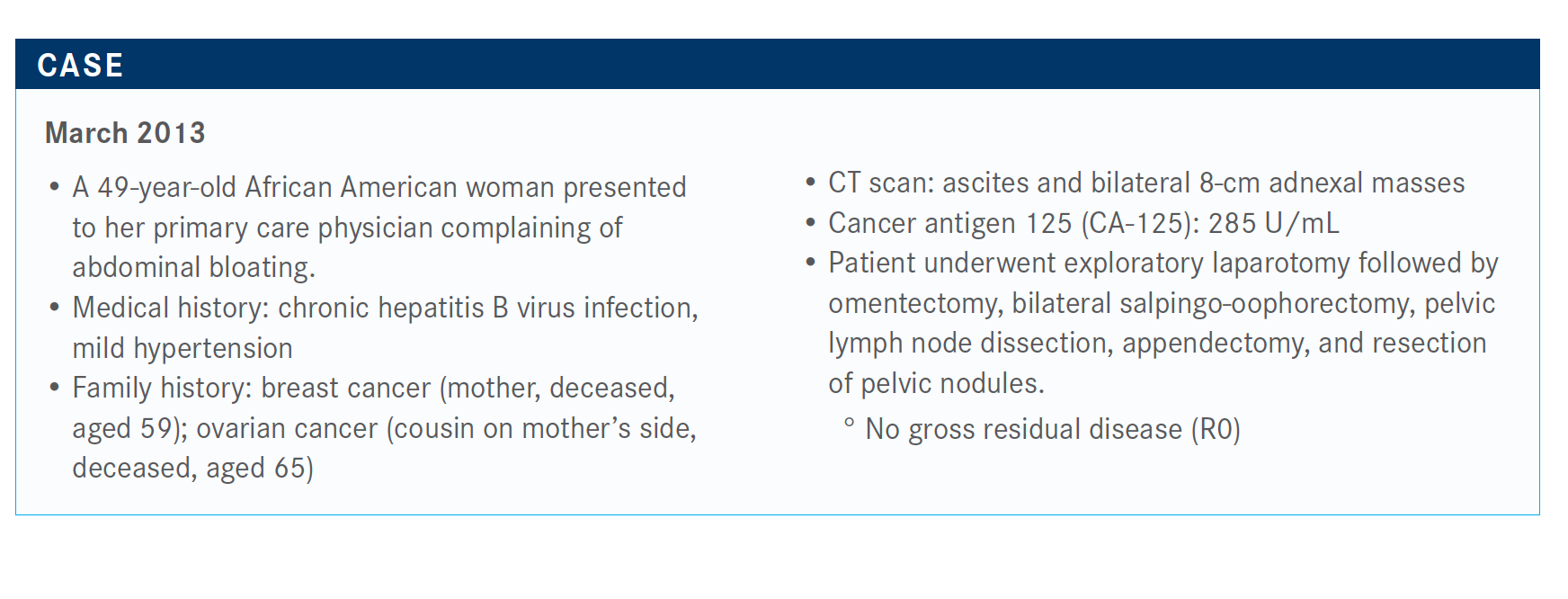
Leslie M. Randall, MD, discussed the case of a 49-year-old African American patients with BRCA-mutated ovarian cancer.


Leslie M. Randall, MD

Leslie M. Randall, MD, professor, Department of Obstetrics and Gynecology, Massey Cancer Center, Virginia Commonwealth University, in Richmond, VA, discussed the case of a 49-year-old African American patients with BRCA-mutated ovarian cancer.

Targeted Oncology™: How do you interpret next-generation sequencing results for mutations that are homozygous or heterozygous based on results from the FoundationOne CDx test?
RANDALL: In terms of heterozygous and homozygous, the BRCA mutation follows the autosomal dominant—the 2-hit hypothesis model, where you had 2 deleted copies of the gene. What your test should be reading is that the patient has a deleterious mutation or does not have a deleterious mutation. Some companies may report it out as either deleterious or not, but that’s what you’re looking for in your report.
Would only the patients with deleterious mutations respond to a PARP inhibitor?
With the niraparib [Zejula] approval, you can use this therapy for all patients.1 It’s not like with the SOLO-1 trial [NCT01844986] of olaparib [Lynparza], [in which] prior approval was restricted to that group.2,3 Now you can expand beyond that; the label for the olaparib/bevacizumab [Avastin] combination is [for patients with] BRCA-mutated homologous recombination deficiency [HRD].4
Are these PARP inhibitors similar in terms of efficacy?
There are some microenvironment differences with niraparib…that might have a differential benefit, but that’s never been proved by a study. The NCCN [National Comprehensive Cancer Network] guidelines are based on the clinical trials that were done….If you look at the recommendations for patients with platinum-sensitive recurrence, 3 of them are approved for the exact same indication; there’s no distinction there.5
Are you using PARP inhibitors in your practice?
There’s so much debate over which one we use and for whom do we use it. I think all in all, niraparib has the broadest indication because it's open to the homologous recombination proficient [HRP] population. Some doctors have decided they will not treat patients who are HRP with a PARP inhibitor.
My personal thoughts are that those subgroups are small. They’re not definitive; they’re not powered to tell us for sure if we should be distinguishing with that [level of granularity].
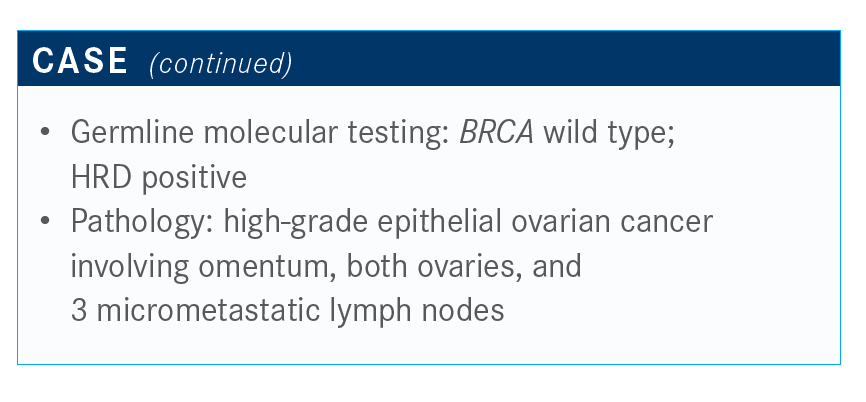
Which genetic tests are good to use in this patient population?
With the Myriad [myChoice CDx] test, you get the patient’s somatic BRCA and the HRD [status] in the same test.6 The FoundationOne test identifies the RAD51C and RAD51D proteins; they’re rare, but you don’t want to miss those.7
With niraparib being approved for all [mutations], the pressure is not as high to detect those different mutations because you can still use it, but it’s nice to know when the patients have those mutations. I think it’s important not to forget to do germline testing. You have to do the germline testing separately. The HRD test does not test for germline BRCA mutations, and that’s what the patients need to know for their own cancer risks and their family to get the cascade testing. That’s important.

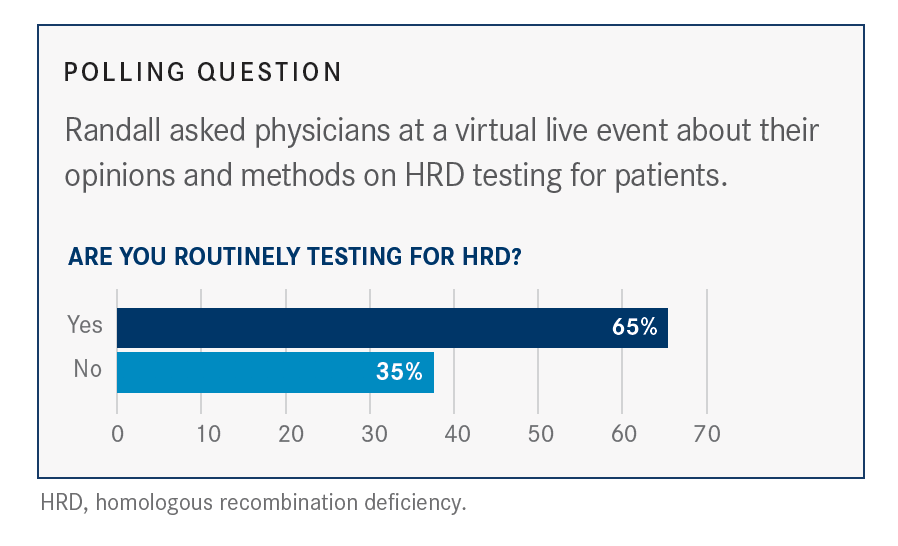
What are your thoughts on HRD testing in this setting, and how do results affect your choice of treatment?
I think the HRD testing will [become more common] based on the outcomes of the [current] studies. I want to give anyone [a PARP inhibitor] who is a candidate for it. It probably works best the sooner that you give it, so if you can get it for them in the front line, [then do so]. I think that’s a reasonable approach.
When a patient’s tumor is positive for a BRCA mutation, which therapy do you use considering the data from the SOLO-1 trial compared with the PRIMA trial (NCT02655016)?
The olaparib and bevacizumab combination and niraparib [labels] both include patients who are germline BRCA mutated.1,8 I’m in the habit of giving them olaparib because we’ve been doing that now for 2 years. Technically you could give them niraparib. I think they’re probably mostly equivalent in terms of efficacy, but in terms of dosing, the niraparib is once a day, so [it’s better] if you have a patient who you don’t think is going to be adherent. There are some tricky things with the niraparib dosing. Now that I have these options, I may offer them whatever is most palatable to them in terms of dosing and schedule.
Would I give them the bevacizumab combination? Probably if I had already started bevacizumab [alone]. A lot of physicians use bevacizumab in our patients who are more high risk, such as our patients with stage IV disease or patients who still have residual disease—especially of any bulk disease—following induction. I would continue those patients on bevacizumab and then probably the PARP inhibitor. I think that’s where I’ll mostly use the combination.
I think we’re learning [because the] data [are] so new and fresh; it’s exciting to have these options. We’ll keep treating patients and come back together at events to talk about our experiences and settle on what we think is best for the patients.
What do the NCCN guidelines recommend for patients without a BRCA mutation?
The NCCN guidelines [say], in the absence of BRCA mutation, the HRD status may provide information of the magnitude of the benefit of PARP inhibitor therapy; now it’s almost prognostic.5

Would you give bevacizumab in frontline treatment for these patients?
When the SOLO-1 data came out, a lot of us had to scramble to get germline or somatic testing done so we could decide if this was a patient who is going to get bevacizumab or not.
In the PAOLA-1 trial [NCT02477644], all the patients had gotten bevacizumab during induction, so [there are no data saying] not to start it during induction but then to start it as maintenance.9 But I think a lot of people are going to end up doing that just for practical reasons, specifically if the patients are on neoadjuvant [therapy], need surgery, and you’re holding bevacizumab the cycle before surgery or holding the bevacizumab the cycle after the surgery—sometimes longer depending on how they’re healing. Sometimes the bevacizumab tends to get omitted from induction just [for] practical purposes.

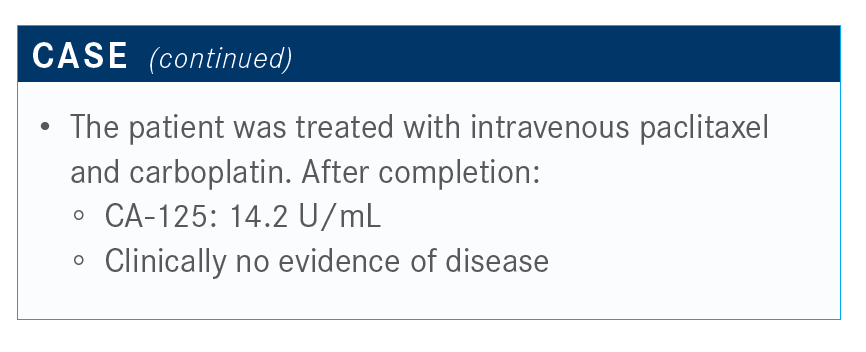
What would you recommend for the patient?
I’m a big proponent of maintenance. Anything we can do to prolong these progression times, especially a well-tolerated oral therapy that [allows] patients to travel and [continue with daily activities], is preferable.
Do you think by prolonging the progression-free survival (PFS) with the PARP inhibitor, you’re maintaining platinum sensitivity?
Yes. There is no question. We know for sure that we extend the proportion of patients who are platinum sensitive; it is definitely higher when you’re using any active maintenance, whether it is bevacizumab or a PARP inhibitor—even more so for PARP. It extends that interval for the patients who are germline BRCA mutated.
It’s interesting because platinum sensitivity is a numerical thing, but it’s also a biological thing. Even if [the patients] make that time interval, do you still behave like a platinum-sensitive patient when you’re retreated with platinum?
We’re starting to get early results of secondary end points of some studies, which are time to the second treatment and the second PFS interval for their first recurrence. There’s no difference between the 2 groups, so there’s no real decrement—but there’s no clear benefit either. None of those studies are powered to detect a difference, so they’re just to try to get a signal to see if there’s some sort of decrement or not, and then to give the reason to study that further. Right now, there’s no signal for a decrement.
How do you monitor patients in the ovarian cancer setting?
The important lab values to watch for are the complete blood count because these PARP inhibitors have the myelodysplastic warning in the labels [and] the liver function tests and their creatinine [levels] at least on a monthly basis.
Normally what I’ll do is order the patient’s CA-125 when I’m getting the monthly labs, but it depends on the patient. We know some patients who develop CA-125 burnout, [so] we’ll order the test every 3 months. If the patient is not on clinical trial, I order imaging tests based on CA-125 symptoms and physical exam, and if anything is off, they’re getting a CT. I don’t do routine imaging because the goal here is to keep people alive for a long time. You don’t want them to be constantly getting scans and radiated. I think that defeats the purpose.
You have some patients in which the CA-125 won’t be a good [prognostic] marker, but in the high-grade serous group, that’s a minority of the patients; most have CA-125 as a good marker.
Can you discuss the recommended niraparib dose adjustments based on baseline bodyweight and platelet count?
In PRIMA, the starting dose of niraparib—this was the prior label for recurrence—was 300 mg per day; that was three 100-mg capsules.8 The first dose reduction was 200 mg per day, and then the second dose reduction is 100 mg per day, and then you’re out of options. You have 3 dose levels for niraparib.
In the NOVA trial [NCT01847274], which was the platinum-sensitive recurrent study, most of the patients needed a dose reduction to at least 200 mg or often even 100 mg.10 [Investigators] went back and [looked at] what factors could have predicted that. What they found [was] body weight less than 77 kg or a baseline platelet count less than 150,000/μL [was] predictive of the need for a dose reduction.
The dose reductions were almost all due to grade 3 or greater thrombocytopenia. This thrombocytopenia can be prolonged and delay the next dose by weeks.
This brings up the concept of individualized niraparib dosing that has been applied in PRIMA based on that data from NOVA.8,10 For those patients who met the criteria, they had to have both 77 kg or above and platelets above 150,000/μL to go on the 300-mg dose, and if they didn’t meet those requirements, then they were started on the 200-mg dose.
If you look at the NOVA data, the incidence of adverse events based on the dose had some significant dose-dependent toxicities. The anemia still remains across the board.10
Niraparib has about a 5% rate of hypertension, and it can be a significant, severe rapid onset and high-grade hypertension. It occurs equivalently across the dose levels.
In the NOVA trial for patients with platinum-sensitive recurrence, the investigators went back and looked at the outcomes for PFS based on these different dose levels. They looked at both the BRCA-mutated group and the nonmutated group and saw no decrement in PFS in the groups whose doses were reduced. These weren’t powered to be definitive analyses, but at the end of the day, most of the patients on this trial could not tolerate the 300-mg dose.
Reference:
1. FDA approves niraparib for first-line maintenance of advanced ovarian cancer. FDA. April 29, 2020. Accessed June 25, 2020. fda.gov/drugs/drug-approvals-and-databases/fda-approves-niraparib-first-line-maintenance-advanced-ovariancancer#:~:text=On%20April%2029%2C%202020%2C%20the,%2Dline%20platinum%2Dbased%20chemotherapy
2. Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2018;379(26):2495-2505. doi:10.1056/NEJMoa1810858
3. FDA approved olaparib (Lynparza, AstraZeneca Pharmaceuticals LP) for the maintenance treatment of adult patients with deleterious or suspected deleterious germline or somatic BRCA-mutated (gBRCAm or sBRCAm) advanced epithelial ovarian, fallopian tube or primary peritoneal cancer who are in complete or partial response to first-line platinum-based. FDA. Updated December 26, 2018. Accessed June 25, 2020. fda.gov/drugs/fda-approved-olaparib-lynparza-astrazeneca-pharmaceuticals-lp-maintenance-treatment-adult-patients
4. FDA approves olaparib plus bevacizumab as maintenance treatment for ovarian, fallopian tube, or primary peritoneal cancers. FDA. Updated May 11, 2020. Accessed June 25, 2020. fda.gov/drugs/drug-approvals-and-databases/fda-approves-olaparib-plus-bevacizumab-maintenance-treatment-ovarian-fallopian-tube-or-primary
5. NCCN. Clinical Practice Guidelines in Oncology. Ovarian cancer including fallopian tube cancer and primary peritoneal cancer, version 1.2020. Accessed June 25, 2020. nccn.org/professionals/physician_gls/pdf/ovarian.pdf
6. myChoice CDx. Myriad. Accessed June 25, 2020. myriad.com/products-services/precision-medicine/mychoice-cdx/
7. FoundationOne CDx technical information. Roche Foundation Medicine. Accessed June 25, 2020. rochefoundationmedicine.com/f1cdxtech
8. González-Martín A, Pothuri B, Vergote I, et al. Niraparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2019;381(25):2391-2402. doi:10.1056/NEJMoa1910962
9. Ray-Coquard I, Pautier P, Pignata S, et al. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. N Engl J Med. 2019;381(25):2416-2428. doi:10.1056/NEJMoa1911361
10. Mirza MR, Monk BJ, Herrstedt J, et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375(22):2154-2164. doi:10.1056/NEJMoa1611310




















