Dorff Discusses the CARD Trial in Metastatic Castrate- Resistant Prostate Cancer
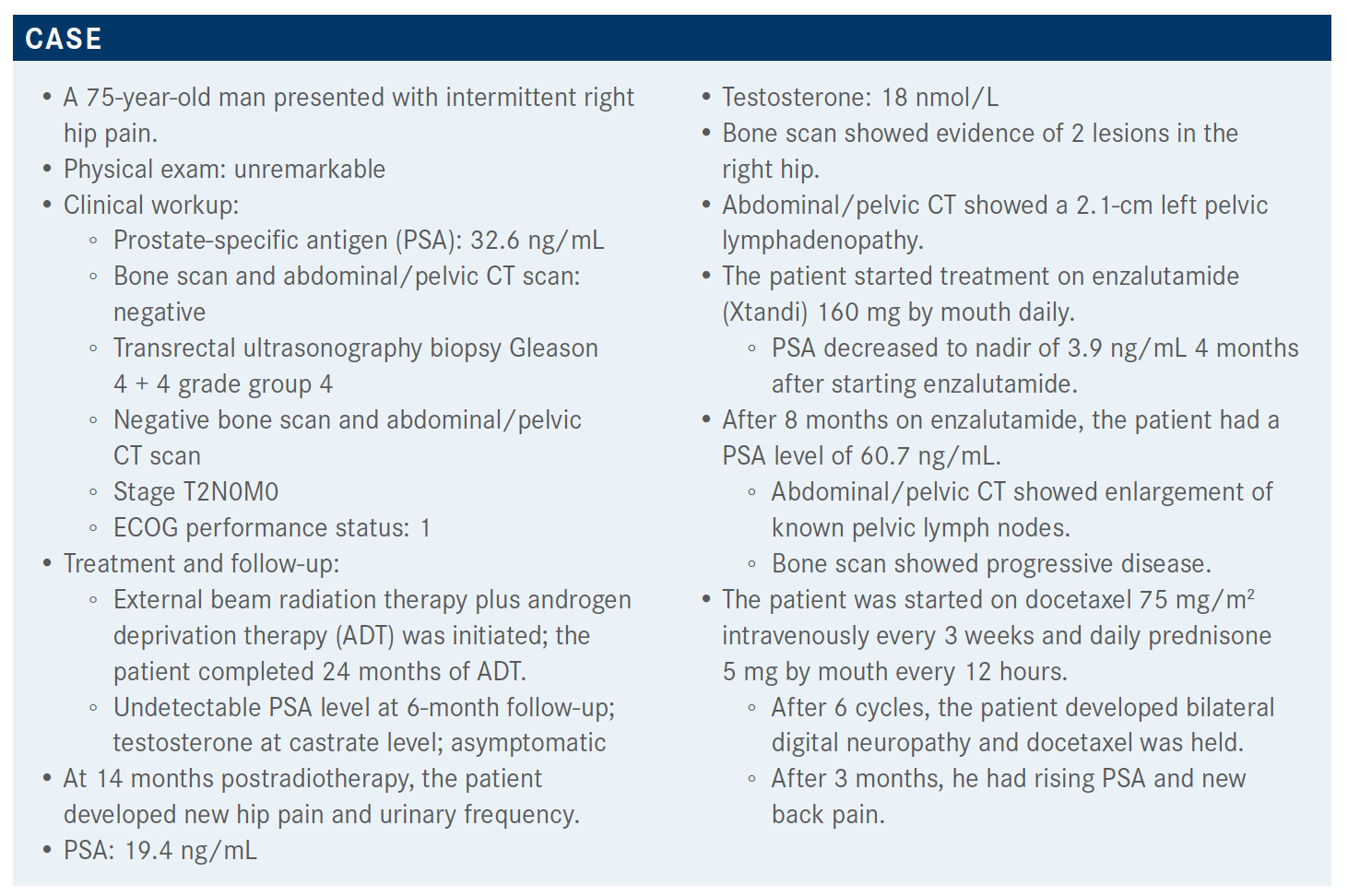
During a virtual Targeted Oncology Case-Based Roundtable event, Tanya Dorff, MD, discussed the case of a 75-year-old man with metastatic castration-resistant prostate cancer.



During a virtual Targeted Oncology Case-Based Roundtable event, Tanya Dorff, MD, head, Genitourinary Cancers Program, and associate clinical professor, Department of Medical Oncology & Therapeutics Research at City of Hope, discussed the case of a 75-year-old man with metastatic castration-resistant prostate cancer.


Targeted OncologyTM: What are some therapeutic options for this patient at this point in his treatment?
DORFF: I think the CARD trial [NCT02485691] was really a practice-changing trial. We had the TROPIC trial [NCT00417079], where we saw the survival advantage of cabazitaxel [Jevtana] compared with mitoxantrone post docetaxel treatment. But I feel like some people still had questions.
The CARD trial randomized men with metastatic castrate-resistant prostate cancer [mCRPC] who had progressed within 12 months on their prior androgen receptor [AR]-targeted agent.1 [This looks at]…how long they responded to their hormone therapy. The other thing that I think is unique about this patient population is one of the ways patients got onto this study: They had to have documented progression, [including] pain progression or symptomatic progression, and 67% of these patients did. It was a pretty aggressive patient population.
Patients were randomized to cabazitaxel at 25 mg/m2 with prednisone and growth factor support versus abiraterone [Zytiga] with prednisone if they had been on enzalutamide or enzalutamide if they had been on abiraterone. This was an open-label study. [I want to] highlight the fact that the cabazitaxel dose in this trial was 25 mg/m2, which is also what it was in the TROPIC trial where they showed the survival advantage. I think many of us have started using 20 mg/m2, and that’s something to discuss. The primary end point was radiographic progression-free survival [rPFS], but they also looked at overall survival [OS].
The patient population is really, I think, representative of who we see. There was a significant percentage of men who were over 75 years old [35% in the cabazitaxel arm and 27% in the abiraterone or enzalutamide arm], and there was less than 20% with visceral metastases in either arm. But, again, the majority had pain. It was a fairly even distribution of abiraterone versus enzalutamide as their first-line therapy and fairly similar across the 2 arms, so the randomization was pretty effective here.
What was the efficacy of the CARD trial?
The primary end point of rPFS [with] cabazitaxel versus the other androgen-targeted agent, abiraterone or enzalutamide, [showed a] significant hazard ratio of 0.54 [95% CI, 0.40-0.73]. The median rPFS was 8 months with cabazitaxel compared with less than 4 months for the abiraterone or enzalutamide arm.
The investigators did a subset analysis. I feel like we rely on these more and more to try to help translate trials to our own practice. Definitely one thing that people ask is about the older population. It was almost half and half for patients over 70 and under 70 years old before they= showed us the 75-year-old cutoff. But the patients over 70 definitely benefited [HR, 0.59; 95% CI, 0.39-0.89]. All the subset analyses that they looked at were positive. The duration of the first androgen deprivation therapy… whether they were on their first AR-targeted agent for less than 12 months or more than 12 months, they benefited from cabazitaxel over the enzalutamide or abiraterone [< 12 months HR, 0.62; 95% CI, 0.39-0.96; ≥ 12 months HR, 0.50; 95% CI, 0.34-0.75]. I think it could be interesting to look at more than just that 12-month cutoff, like really quick progressors and really long responders, but these are the data we have.
OS was also in favor of cabazitaxel in this trial, with a median OS of 13.6 months versus 11 months [for cabazitaxel vs abiraterone or enzalutamide (HR, 0.64; 95% CI, 0.46-0.89)]. That feels kind of short to me, which is why, when we were looking at the entry criteria, I was mentioning that more than 60% of patients got on the trial with pain progression. I think that’s a more aggressive population, and that might account for why there’s a lower survival than what you might expect if patients just had PSA rising and nothing changing on scans and no pain. That’s a different group of patients.
In terms of responses, I think this was also very informative. PSA response defined as 50% reduction or more was definitely higher with cabazitaxel, 35.7% versus 13.5% with the second hormone agent—not 0% [response]. PSAs go down but only in 13.5%. That’s definitely lower than when you use the abiraterone or the enzalutamide the first go-around.
Objective response rate was 36.5% for cabazitaxel; that’s pretty high in my view. I find that pretty compelling versus 11.5% for abiraterone or enzalutamide—not 0% but definitely lower. Then pain response—these patients are coming on with pain. Pain relief is definitely a major secondary goal besides prolonging their survival. Pain response was 45% versus 19%, [respectively]. Cabazitaxel was superior versus the other AR-targeted agent in all of these different parameters, [including] time to symptomatic skeletal events, so not just seeing an asymptomatic fracture on a scan but a fracture that caused pain or needed intervention was also improved. These are all really clinically meaningful.
How were patients affected by adverse events (AEs) on this study? What was their quality of life?
Now, that’s the big caveat. We worry about our older, more frail patients—can they really tolerate cabazitaxel? There were about twice as many treatment discontinuations due to AEs on the cabazitaxel arm [19.8% vs 8.9% with abiraterone or enzalutamide], but there was not a signal of more deaths [5.6% vs 11.3%]. Grade 3 and higher AEs were similar [56.3% vs 52.4%], which suggests that much of that may be driven by the cancer and not necessarily the treatment. Serious AEs also similar on the 2 arms [38.9% vs 38.7%], which was very interesting.
For health-related quality of life, there was a lower probability of deterioration with the cabazitaxel, probably because it’s controlling the cancer. Much of quality of life in these patients who were more heavily pretreated, with more aggressive prostate cancer, was cancer related, and so more effective treatment led to better quality of life. I think that’s a really important thing I like to talk to my patients about because they often assume that they’re going to feel worse on chemotherapy. I like to blow their minds and say: “You’re feeling sick from your cancer. You’re going to feel better when we get you on chemotherapy and it starts working.”
I think these are important data that people should see. I was surprised by how much these data influenced my practice.
Do you think there are biases when it comes to the AEs of oral treatments versus other types of therapies?
Yes, I think there is some bias.…I definitely have a lot of patients who come in with a strong opinion, and sometimes I can persuade them with something like the CARD data and sometimes I can’t. We do our best to inform them. Even if they choose the abiraterone or the enzalutamide, there was less than 20% PSA response and 11.5% objective response, and about 20% pain relief; it wasn’t 0% so that you could say, “Look, I don’t have a lot of confidence in this. The data suggest that the chemotherapy is the better route, but if you need a few months off before you consider plunging into more chemotherapy, we’ll do it.” You set their expectation to what the data show. Then I think we could also point to the quality-of-life data and say, “Look, quality of life is preserved more on the chemotherapy arm because the cancer is driving the AEs that you’re feeling right now.”
What do you think about the mCRPC landscape overall at the moment?
The biology of mCRPC is complex, so there is heterogeneity, I would argue, not just of the different cancers but also of the people that we treat. Therapeutic sequencing is [complex]. There’s not 1 right answer. We have to make these complex decisions and weigh different factors and different data sets. Androgen deprivation is a cornerstone, even though new therapies are emerging. But switching the mechanism of action when it comes to the next-generation hormonal therapies is associated with improved survival.
Reference:
1. de Wit R, Kramer G, Eymard JC, et al. CARD: randomized, open-label study of cabazitaxel (CBZ) vs abiraterone (ABI) or enzalutamide (ENZ) in metastatic castration-resistant prostate cancer (mCRPC). Ann Oncol. 2019;30(suppl 5):v851-v934. doi:10.1093/annonc/mdz394.040






















