Carducci Discusses CARD Trial Data for Metastatic Castration-Resistant Prostate Cancer
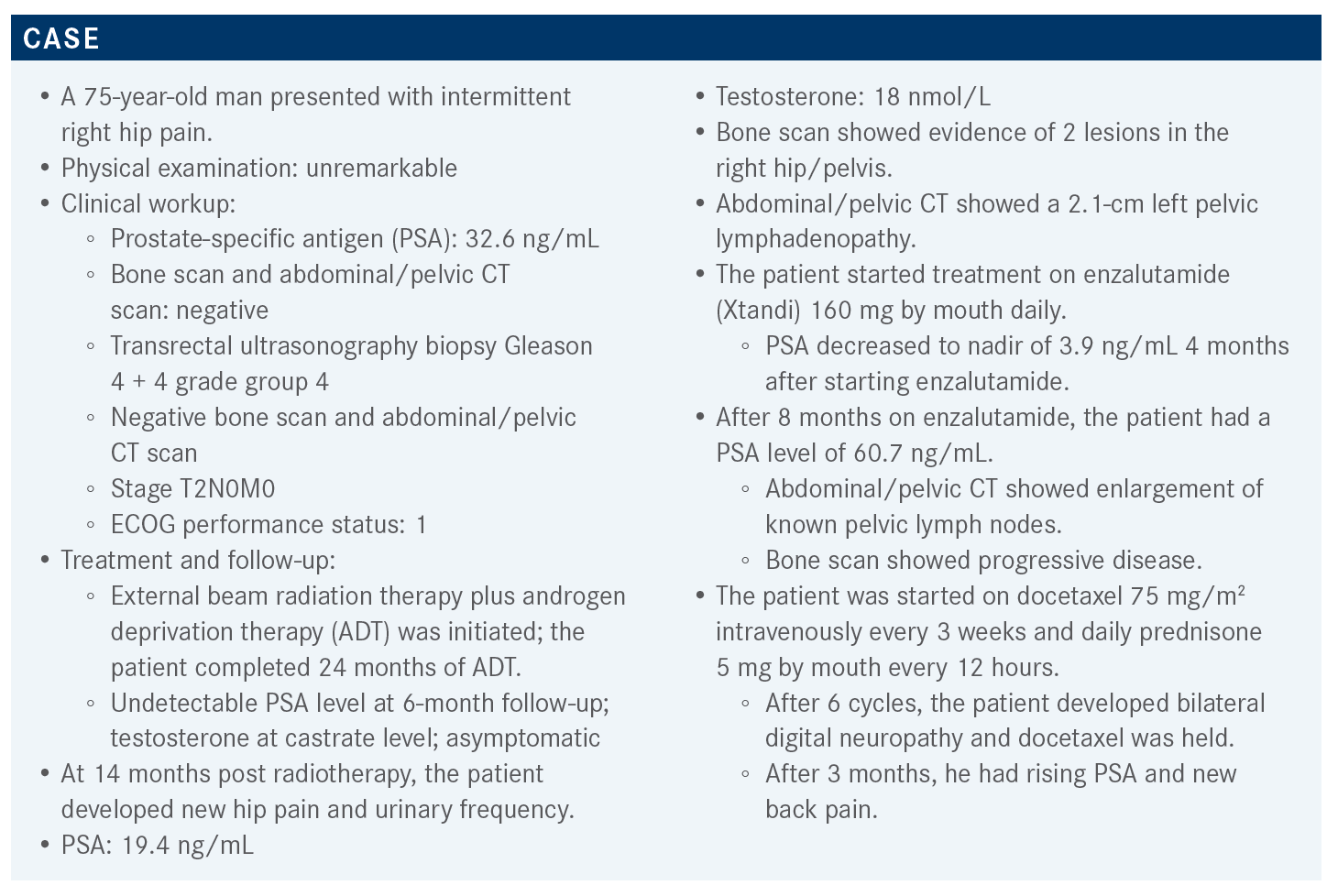
During a virtual Targeted Oncology Case-Based Roundtable event, Michael A. Carducci, MD, reviewed the results of the CARD trial to support his recommendation of cabazitaxel for the treatment of a 75-year-old man with metastatic castration-resistant prostate cancer.



During a Targeted Oncology Case-Based Roundtable event, Michael A. Carducci, MD, AEGON professor of Prostate Cancer Research, associate cancer center director for Clinical Research. regional research director for the National Capital Region at Johns Hopkins Sidney Kimmel Cancer Center, reviewed the results of the CARD trial to explain his recommendation of cabazitaxel (Jevtana) for the treatment of a 75-year-old man with metastatic resistant prostate cancer.




Targeted OncologyTM: What guidelines are available for prostate cancer?
CARDUCCI: The recent American Urological Association, American Society for Radiation Oncology, and Society of Urologic Oncology recommendations as to what you might do in this setting are listed like the National Comprehensive Cancer Network guidelines in terms of having many options.1 They are always telling us to think about sequencing our agents, which is what we are talking about. Patients with symptomatic bone metastases might benefit from radium, [as well as] those who do not have any visceral disease. Cabazitaxel [Jevtana] would be an option to move to. If they have a suspected deleterious germline or somatic mutation in homologous recombination repair genes, then you look at PARP inhibitor or pembrolizumab [Keytruda]. The only other thing the guidelines have added is that you could think about platinum therapy in combination with other chemotherapy if the patients have DNA repair enzyme deficiency.
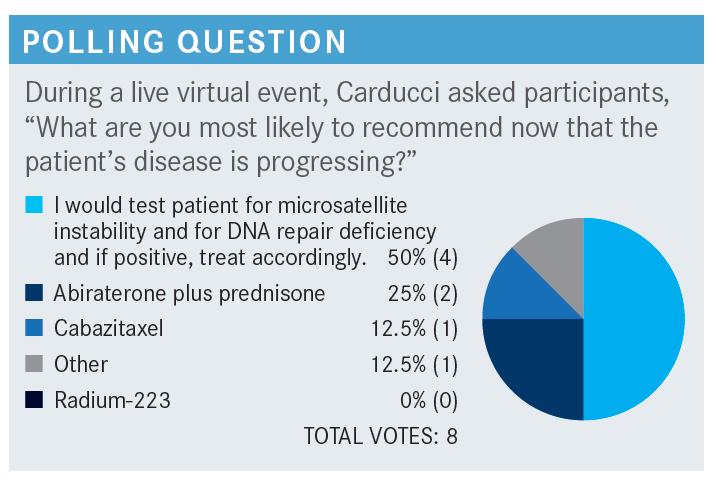
How would you sequence therapies for this patient?
After patients have enzalutamide [Xtandi], moving to abiraterone [Zytiga] is not likely to work. If they have abiraterone first, and then move to enzalutamide, it is not likely to work. And yet this patient has just had chemotherapy; he already had 2 lines of therapy [with enzalutamide and then docetaxel/prednisone], so you must make a choice because he is still doing fairly well.
The CARD study [NCT02485691] was done to help us sort that [out].2,3 These patients had metastatic castrate-resistant prostate cancer [mCRPC] and had progressed in the last 12 months after their prior intensified hormonal therapy. They could have had docetaxel [before or after abiraterone or enzalutamide] as well. Patients were randomized to get cabazitaxel versus whichever androgen receptor targeted agents [ARTA] that they didn’t have previously. So if they had enzalutamide before, they would now have the possibility of getting abiraterone as their choice and vice versa. Investigators were looking for radiographic progression-free survival [rPFS], secondary end points of overall survival [OS], symptomatic skeletal events, [PSA response, tumor response, safety, health-related quality of life, and biomarkers]. This is a study looking at what is the right next option.
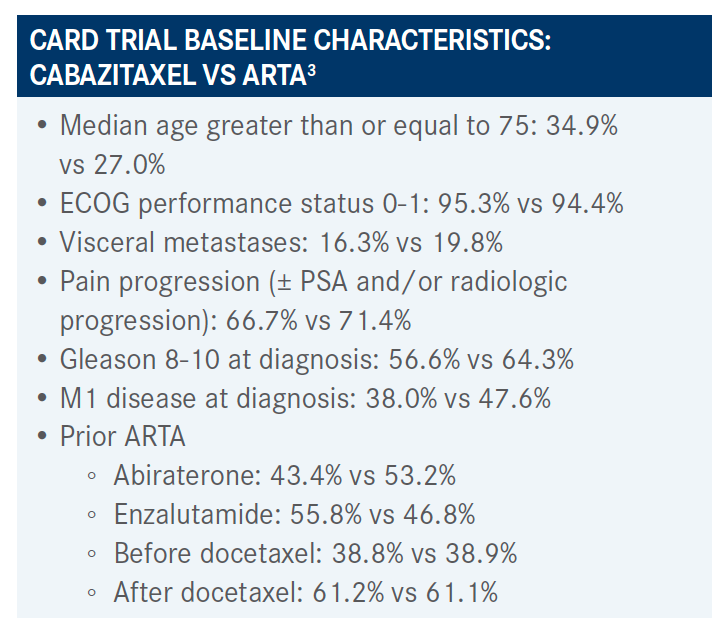
What were the patient’s baseline characteristics in this study?
About 35% of these patients were over 75 years old [in the cabazitaxel arm]. Prostate cancer is a disease of aging, so we’re often treating older men, making decisions about these therapies, and adverse effects [AEs] of tiredness, fatigue, chemotherapy, and the like. In the CARD study, about 70% of the patients were symptomatic with pain [with cabazitaxel]. About 40% presented with metastatic disease as compared with this patient who developed it under our watch. Patients’ choice of a first-line therapy— abiraterone to cabazitaxel or enzalutamide—was in the range of 43.4% or 53.2%, in that order. It was pretty typical of how we treat for this patient that we have today.


How did patients do in the CARD trial?
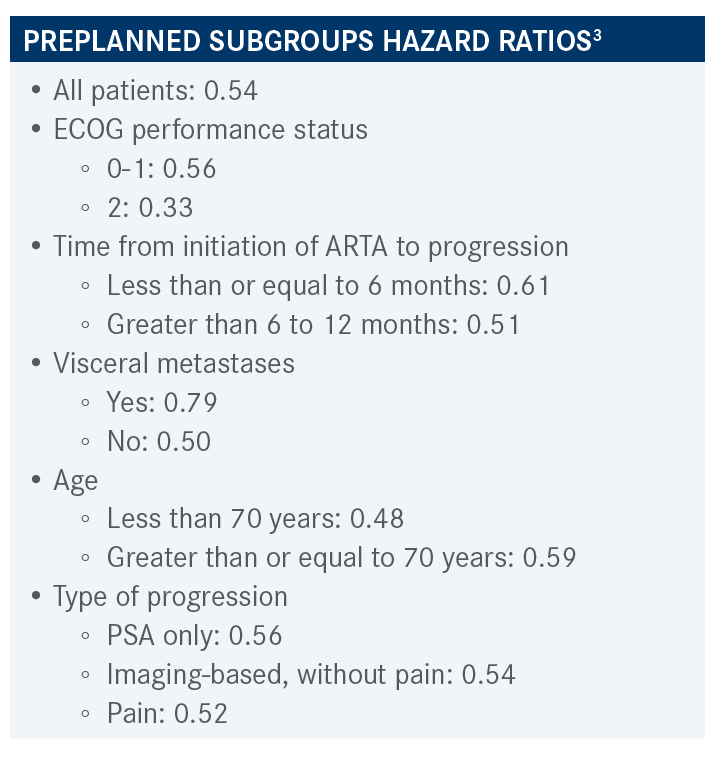
Looking at the primary end point, there was a 4.3-month difference in rPFS [median, 8.0 vs 3.7 months] and a hazard ratio of 0.54, so a 46% reduction in risk of progression by radiographic [scans]. That was statistically significant.
All the preplanned subgroups favored the cabazitaxel arm—in terms of age, if they’ve had a time since their last disease [progression], visceral metastases, everybody seemed to benefit more with the cabazitaxel. There was bit of crossing over the 1.00 line in the poor performance status population, those with visceral metastases, and people progressing by PSA only, but the overall trend was in favor of cabazitaxel.


What was the efficacy of cabazitaxel for the secondary end points?
The OS data were also significant, but in this case 2.6 months’ improvement in survival for cabazitaxel over ARTA [median, 13.6 vs 11.0 months], a 36% reduction in risk of death [HR, 0.64; 95% CI, 0.46-0.89; P = .0078]. This was statistically significant, suggesting that choosing cabazitaxel for this selected patient population [is appropriate]. PFS had about 2 months’ difference [median, 4.4 vs 2.7 months], a 48% reduction in risk of progression; another statistically significant end point in this study.
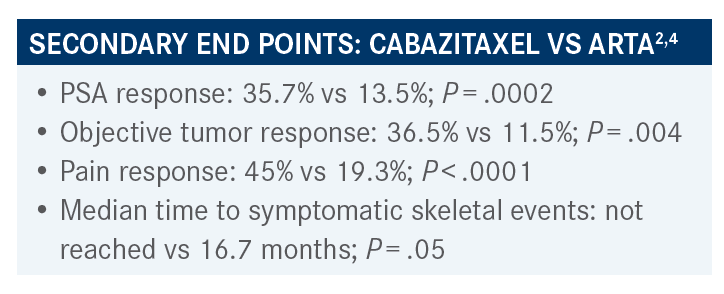
PSA response was higher for patients with cabazitaxel, and objective tumor response was higher for cabazitaxel.2,4 Those having pain and getting a response was higher for cabazitaxel. The time to symptomatic skeletal events was longer for those on the cabazitaxel, suggesting [that] for second-line hormonal therapy in this case clearly cabazitaxel wins in this study.


Please describe the toxicity and quality-of-life profile in CARD.
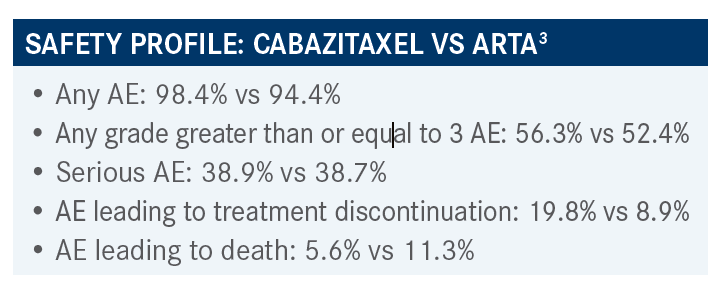
There were higher toxicity rates in terms of AEs leading to treatment discontinuation with cabazitaxel, about 20%.2,3 About 9% AE [on ARTA] leading to discontinuation, but generally everyone had an AE of some sort. Grade 3 or greater was equal, same with serious AEs. There was less in terms of AEs relating to death to cabazitaxel.
Looking at quality of life, all these patients eventually progressed, so these data are always hard to detail what it means. But looking at the Functional Assessment of Cancer Therapy-Prostate [responses], I think it shows that the cabazitaxel arm tended to keep their quality of life longer.5 When you look at the trends over time, it went down over time but in general, the cabazitaxel arm had higher-scored quality of life.


What do you think of this patient’s case in comparison to the mCRPC setting as a whole?
I think we are learning a lot and most of us have a sense of time [for sequencing] that this biology is complex. Here is an individual whose metrics were earlier than average— that is time to [progression], castration resistant on enzalutamide and such. I think we are still trying to sort out that biology [of the disease] to help with management and I think when we first came out with all of these drugs earlier this last decade [we were unsure]; we have a number of agents now and I think all of us have a flow [of how we use them].
I think the CARD study helps us to figure out when to use what and clearly suggests that second-line hormonal therapy in this case has limited activity and other medicines that are out there, even immune-oncology, is trying to go against them because the activity seems to be quite limited.
References:
1. Lowrance WT, Breau RH, Chou R, et al. Advanced prostate cancer: AUA/ASTRO/SUO guideline part I. J Urol. 2021;205(1):14-21. doi:10.1097/JU.0000000000001375
2. de Wit R, Kramer G, Eymard J, et al. 3965 - CARD: randomized, open-label study of cabazitaxel (CBZ) vs abiraterone (ABI) or enzalutamide (ENZ) in metastatic castration-resistant prostate cancer (mCRPC). Ann Oncol. 2019;30(suppl 5):v851-v934. doi:10.1093/annonc/mdz394
3. de Wit R, de Bono J, Sternberg CN, et al; CARD Investigators. Cabazitaxel versus abiraterone or enzalutamide in metastatic prostate cancer. N Engl J Med. 2019;381(26):2506-2518. doi:10.1056/NEJMoa1911206
4. Fizazi K, et al. Pain response and health-related quality of life (HRQL) analysis in patients with metastatic castration-resistant prostate cancer (mCRPC) receiving cabazitaxel (CBZ) versus abiraterone or enzalutamide in the CARD study. Presented at: Genitourinary Cancers Symposium; February 13-15, 2020; San Francisco, CA. Accessed April 6, 2021. https://bit.ly/3ws7Qad
5. Fizazi K, Kramer G, Eymard JC, et al. Quality of life in patients with metastatic prostate cancer following treatment with cabazitaxel versus abiraterone or enzalutamide (CARD): an analysis of a randomised, multicentre, open-label, phase 4 study. Lancet Oncol. 2020;21(11):1513-1525. doi:10.1016/S1470-2045(20)30449-6

















Survivorship Care Promotes Evidence-Based Approaches for Quality of Life and Beyond
March 21st 2025Frank J. Penedo, PhD, explains the challenges of survivorship care for patients with cancer and how he implements programs to support patients’ emotional, physical, and practical needs.
Read More




