Vesole Discusses the Benefits and Challenges of Daratumumab in Patients With NDMM
At a live virtual event, David H. Vesole, MD, PhD, explained to other clinicians the use of daratumumab in the treatment of patients with newly diagnosed multiple myeloma who are either eligible or ineligible for autologous stem cell transplant.


David H. Vesole, MD, PhD
At a live virtual event, David H. Vesole, MD, PhD, director, Myeloma Program at MedStar Georgetown University Hospital, professor of Medicine at Georgetown University in Washington, DC, and the co-director, Myeloma Division and director of Myeloma Research at John Theurer Cancer Center, explained to other clinicians the use of daratumumab (Darzalex) in the treatment of patients with newly diagnosed multiple myeloma (NDMM) who are either eligible or ineligible for autologous stem cell transplant (ASCT).
Vesole also looked at the challenges of adding daratumumab to a regimen for a patient eligible for transplant and the benefits of administering the treatment subcutaneously.
Treating Transplant-Eligible Patients
Benefits of Choosing Transplant in Patients With Newly Diagnosed Multiple Myeloma
David H. Vesole, MD, PhD: I’m fortunate to be on a committee for the international transplant registry, and we published an article in Cancer looking at different age cut offs [during treatment].1 Was it safe? Was it effective? And did the patients have good long-term outcome? We looked at about 16,000 transplant [procedures] in North America over the past 10 years. [About] 2200 of them were patients over 70 years old, so we looked at over 70 vs less than 70 years old and the mortality rate was less than 1%. The response rate was identical. The progression-free survival [PFS] was identical for patients over and under 70 years old. Patients over 70 died, so the overall survival [OS] was shorter because they had other comorbidities and medical conditions over time.
We did another part of these data; the paper just got accepted in Cancer and looked at this group that was over 75 years old.2 It went from 2200 [patients who] were over 70 down to 450 who were over 75. [We saw the] same outcome. Now this is a very select group of patients that are handpicked, because only a smattering of those patients was over 75, but we looked at those 450 patients and the transplant-related mortality was still less than 1%. The response rates and the PFS were like those [younger] patients. So, age [by] itself is not a reason not to transplant.
Now, the latest [trend] is to give daratumumab with bortezomib [Velcade], lenalidomide [Revlimid], and dexamethasone [D-VRd]. I think most [physicians] would agree that triplets or quadruplets are the standard of care for a transplant-eligible patient. We’re also going to talk about transplant-ineligible patients, and how to manage them. The number of treatment cycles varies in the ASCO [American Society of Clinical Oncology] guidelines. The comments from the experts, if you will, was 2 to 4 cycles. I will tell you, however, that I generally treat until they hit a plateau. With current regimens, you give D-VRd or KRd [carfilzomib (Kyprolis), lenalidomide, and dexamethasone], and most [patients] plateau by the third cycle. But I rarely give a 4-cycle therapy. I’m not fixated on the number of cycles. I look at their response to the therapy, and then decide whether I should move them on to transplant.
Phase 3 CASSIOPEIA Trial (NCT02541383) Results
This used VTd [bortezomib, thalidomide (Thalomid), dexamethasone], transplant consolidation, and then there’s a randomization, which is not important because I want to focus on the quadruplet therapy. [That quadruplet therapy is] daratumumab-VTd [D-VTd], transplant, followed by D-VTd, and then daratumumab maintenance.1
So, quadruplet vs triplet with the same basic schema. There were 1000 patients in this trial, and the quadruplet beats the triplet, even though [both groups would] get transplants. When they looked at minimal residual disease [MRD] negativity, using next-generation flow cytometry and next-generation sequencing [NGS]; in either instance, the 4-drug regimen had a superior MRD negativity compared [with] the 3-drug regimen, [64% vs 44% using flow cytometry and 57% vs 37%, respectively].


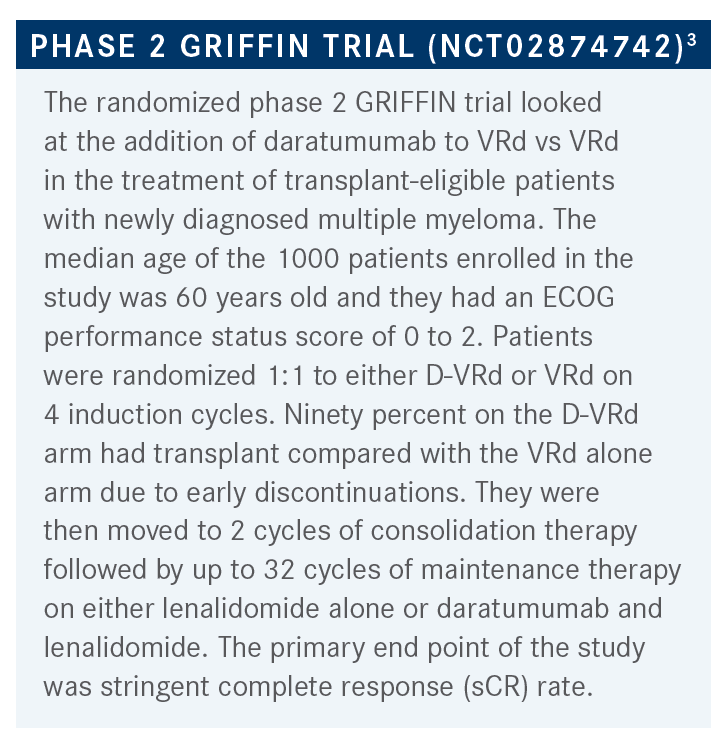
Outcomes of the GRIFFIN Trial
This is the same basic concept except we’re going to give them lenalidomide instead of thalidomide. [So, the treatment options are] D-VRd vs VRd. Patients get the induction for 1 to 4 cycles, they get a transplant, they get consolidation for 2 cycles, then they get randomized to daratumumab plus lenalidomide if they had daratumumab originally. There’s no crossover here. When you look at the D-VRd, the complete remission rate is 82% and when you look at the VRd alone, the combination is 61%. So it was a 20% improvement in the depth of response by giving D-VRd.3
Regarding sCR, the 4 drugs beat the 3 drugs, and when you look at the MRD negativity, the 4 drugs beat the 3 drugs, 62% vs 27%, respectively. It’s a very potent regimen to give the quadruplet vs the triplet. When they did this, again, the follow-up—which is not yet published, this is only presented as an abstract, so follow-up is not that long yet—but when they looked at the 24-month PFS rate, it’s not much different yet, and the OS is going to take years to show a difference.
When you give daratumumab on top of lenalidomide, I just want to point out that the neutropenia is higher when you give daratumumab, as it does cause neutropenia. Grade 3/4 neutropenia with the quadruplet, it’s 41% vs 22% with the triplet. The rest of the numbers are not that much different between the 2 groups, thrombocytopenia is a hair higher, but it’s mainly neutropenia that is significantly higher when you give daratumumab with lenalidomide.
Deciding the End Points When Looking at Salvage Therapy in Multiple Myeloma
I almost guarantee the OS will not be different between [other] studies, because we can salvage them with whatever they received. Back in the day, the FDA would only approve drugs based on OS, but because we now have so many salvage therapies, not just for myeloma, but breast cancer, lung cancer, etc., you can’t really use OS because [we’re looking at] salvage therapies. You have to use the depth of response in this case, or the PFS, so most of the current myeloma trials use MRD negativity as their end point.
Our group believes in KRd, but even then, we don’t give D-KRd because we can’t get it approved. Even if we could, I’m not sure that I’d rather give it now, because I’d rather use it as salvage therapy. The depth of response is better. If I did a D-KRd treatment vs KRd there’s no doubt that you get a deeper response with the 4-drug regimen vs 3-drug regimen. Moreover, MRD negativity is a surrogate marker, but it really is a good predictor of remission duration, even if it doesn’t predict OS.
Challenges With Adding Daratumumab and Continuing to Transplant
In the paper we submitted, in the over 75-year-old population doing transplant, the reviewer [pointed out that] if you look at daratumumab, lenalidomide, and dexamethasone [DRd] in the frontline setting, the response rate [was durable through 45 months]. [The reviewer commented,] if you can do that with DRd, why would we bother doing a transplant? I had to answer the reviewer, so I went back and looked at [these data and] the 2-year PFS rate with D-VRd, because that’s when I had the data on, [it was a] 95% 2-year PFS rate.
With DRd without a transplant it was 80%, so is that a difference? A 15% difference in that larger population is significant, even though you’re comparing across trials. But, to me, I think that really transplants shouldn’t be going away because we have such effective salvage therapy.
The reviewer also mentioned that cost is an issue, [and recent comments showed that giving daratumumab upfront] is probably not cost effective, but as far as the duration of response, you’re good because you can [use] salvage therapy for these patients.
These are unanswered questions of what the most cost-effective medicine really is. In the United States, it’s not a concern. Outside the United States, it is a major concern, and should everyone get treated with quadruplets? Because there’s no doubt that the depth of response is better.
Treating Transplant-Ineligible Patients


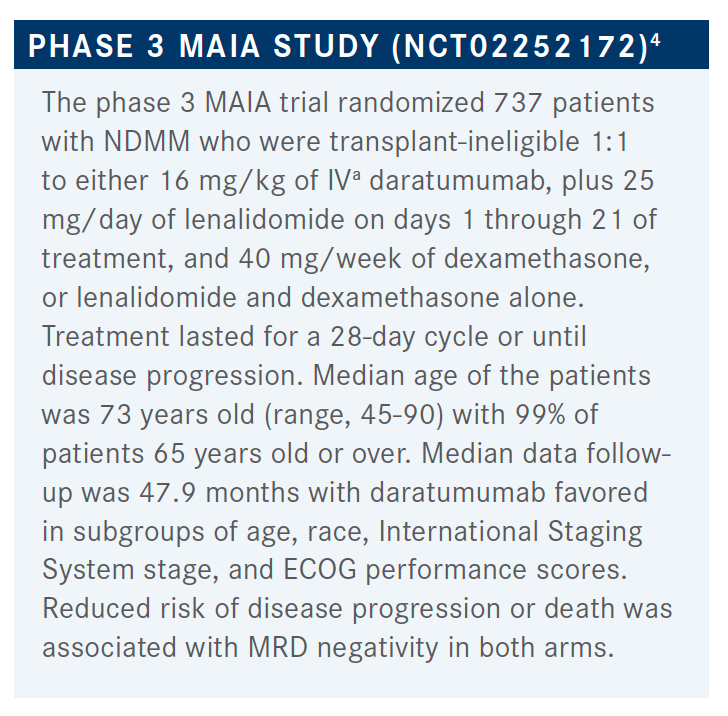
MAIA Study Efficacy and Safety Outcomes
On the DRd arm, we’re at 44 months compared with 41 months in VRd; at 4 years, the PFS rate is still 60%.5 So the PFS is going to be more than 48 months vs 41 months for VRd. [The DRd regimen has a longer PFS] and it’s got a better overall response rate, [compared with VRd] in the 80% range to 93%, so DRd has higher and more durable responses. Just keep that in mind when you have an older individual, and you don’t get any peripheral neuropathy.
Even given once a week, or 3 weeks out of a month, you still get peripheral neuropathy even as the DRd regimen has deeper responses, longer responses than giving VRd when you try to compare across studies. While 60% of the patients were still in remission, the PFS has not been reached at 48 months, but it was far superior to the Rd. [These data are a given because] triplets essentially always beat doublets. This was true regardless of age, whether you’re younger than 75 or over 75 years old, all these data favored the triplet vs the doublet.
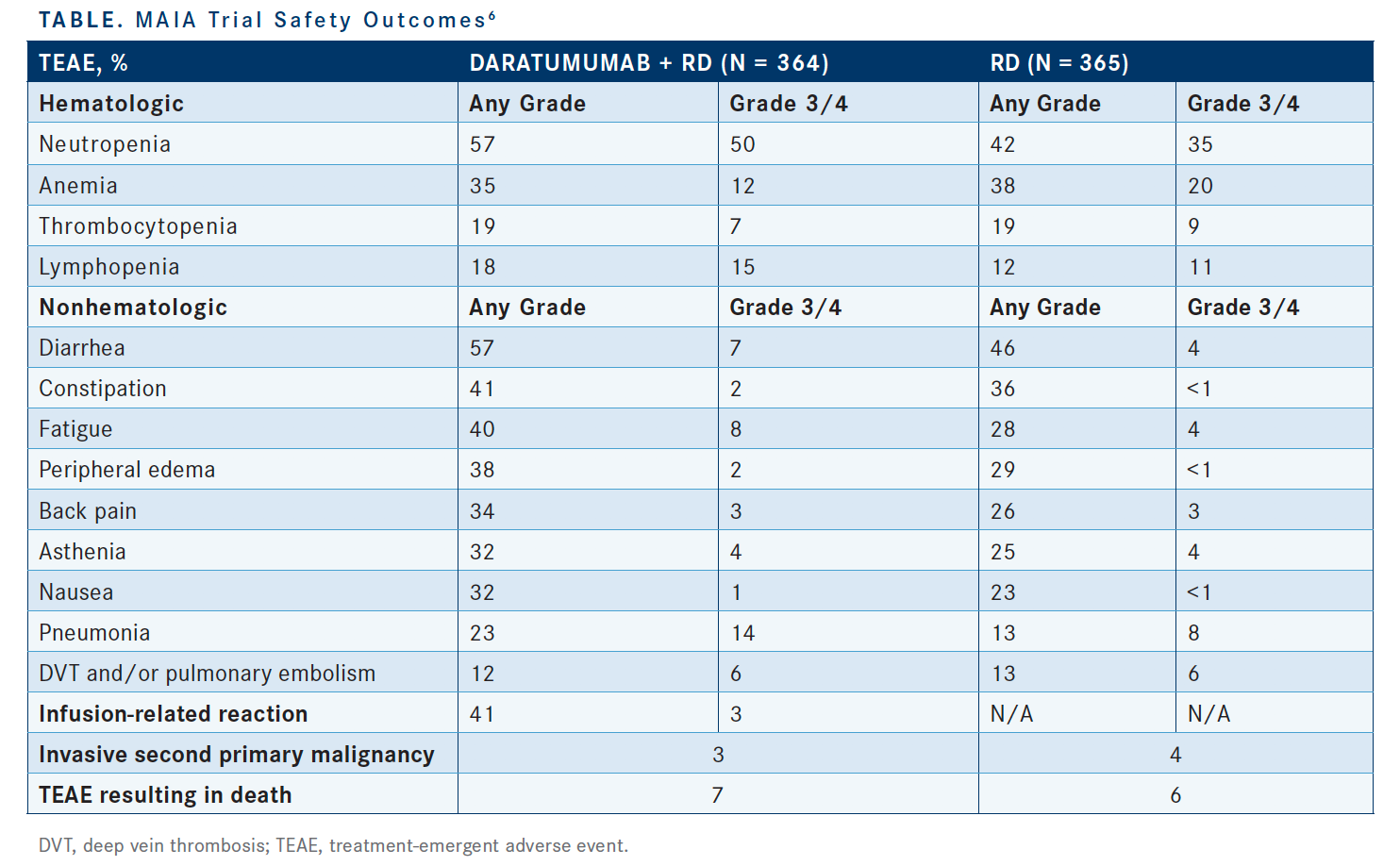
When you give daratumumab with lenalidomide you get more neutropenia, grade 3/4 is 50% vs 35% for Rd alone (table6). The rest of the toxicities are comparable between the 2, but because you do get more neutropenia, you do get more infectious complications with the triplet vs the doublet.


Giving Daratumumab Subcutaneously vs Intravenously
The COLUMBA trial [NCT03277105] was what led to the subcutaneous formulation approval by the FDA.7 They took the original indication for daratumumab as a single agent for patients with relapsed/refractory disease. Relapsed/ refractory single agent [was given to patients with] 3 or more lines of prior therapy, half [received daratumumab] subcutaneously and half got it intravenously [IV].
They were looking for the response rate, as well as infusion reactions, which showed a difference between the 2 in a large trial of about 500 patients. What researchers found was that the response rates were identical between the subcutaneous and the IV delivery across the board. It was a noninferiority trial, and they proved it was noninferior, they were giving the daratumumab over 5 minutes. The toxicities were 25% to 30% infusion toxicities with the IV, and 10% to 12% in the subcutaneous arm.
There was another subcutaneous trial and if you look across the trials, the infusion reaction rate with IV daratumumab is about 30% diffusion, or the injection administration and reaction rate with subcutaneous is 11%. So, it’s safer, it’s faster, and the efficacy is identical. We converted 98% of our patients to subcutaneous treatment and all our newly started patients for months and months now are getting [treatment this way]. We still have a few older patients on IV, who just refuse because they say, “Well, this one’s working fine. Why would I want to change?” They just refuse to change to the IV. We’ve never had to switch someone back and forth.
REFERENCES
- Moreau P, Attal M, Hulin C, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): a randomised, open-label, phase 3 study. Lancet. 2019;394(10192):29-38. doi:10.1016/S0140-6736(19)31240-1
- Munshi PN, Vesole D, Jurczyszyn A, et al. Age no bar: A CIBMTR analysis of elderly patients undergoing autologous hematopoietic cell transplantation for multiple myeloma. Cancer. 2020 Dec 1;126(23):5077-5087. doi:10.1002/cncr.33171
- Kaufman JL, Laubach JP, Sborov D, et al. Daratumumab (DARA) plus lenalidomide, bortezomib, and dexamethasone (VRd) in patients with transplant-eligible newly diagnosed multiple myeloma (NDMM): updated analysis of Griffin after 12 months of maintenance therapy. Blood. 2020;136(suppl 1):45-46. doi:10.1182/blood-2020-137109
- Perrot A, Lauwers-Cances V, Cazaubiel T, et al. Early versus late autologous stem cell transplant in newly diagnosed multiple myeloma: long-term follow-up analysis of the IFM 2009 Trial. Blood. 2020;136(suppl 1):39. doi:10.1182/blood-2020-134538
- Voorhees PM, Kaufman JL, Laubach J, et al. Daratumumab, lenalidomide, bortezomib, and dexamethasone for transplant-eligible newly diagnosed multiple myeloma: the GRIFFIN trial. Blood. 2020;136(8):936-945. doi:10.1182/blood.2020005288
- Facon T, Kumar S, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N Engl J Med. 2019;380(22):2104-2115. doi:10.1056/ NEJMoa1817249
- Mateos MV, Nahi H, Legiec W, et al. Subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma (COLUMBA): a multicentre, open-label, non-inferiority, randomised, phase 3 trial. Lancet Haematol. 2020;7(5):e370-e380. doi:10.1016/S2352-3026(20)30070-3






Survivorship Care Promotes Evidence-Based Approaches for Quality of Life and Beyond
March 21st 2025Frank J. Penedo, PhD, explains the challenges of survivorship care for patients with cancer and how he implements programs to support patients’ emotional, physical, and practical needs.
Read More



