Roundtable Discussions: Alumkal Reviews Challenges in a Case of mCRPC
During a Targeted Oncology Case-Based Roundtable event, Joshi Alumkal, MD, discussed the case of a 75-year-old man with metastatic castration-resistant prostate cancer.


Joshi Alumkal, MD

During a Targeted Oncology Case-Based Roundtable event, Joshi Alumkal, MD, discussed the case of a 75-year-old man with metastatic castration-resistant prostate cancer (mCRPC).






ALUMKAL: Are there any concerns about the patient’s management so far?
MIRMIRAN: I think his management has been appropriate.
AL-JANADI: I don’t think it has been [appropriate]. I don’t think the [right hip pain was investigated enough [after having a negative bone scan].
ALUMKAL: A CT scan was done which didn’t show any concerning lesions in the right pelvis.
AL-JANADI: They should have probably done a sodium fluoride PET scan too.
ALUMKAL: Certainly with molecular imaging one can find lesions that would not be apparent on conventional imaging. But, for a symptomatic lesion, it’s very common to see findings on conventional imaging, whether it’s CT scan or bone scan. So, I can’t really fault them for pursuing this mode of imaging. Unfortunately, he had metastatic disease [in the right hip and] another area.
A. CHOWDHARY: If they had done a PET scan and picked up some of these lesions earlier, would it have changed the management or even changed his disease course? I really doubt it would. I think that we’re reaching for the PET scan more often than we should. I don’t think it changes his management and long-term outlook majorly. Conventional imaging in most of these cases is all you need.
FRONTIERA: Did the patient get a course of radiation therapy that he wouldn’t have needed?
AL-JANADI: Exactly. I think we’re biased against [PET scan] because we reach for it in every single malignancy. If the goal is accurate staging, I think we should use all tools at our disposal for accurate staging. It’s important to accurately stage a case.
ALUMKAL: If he had molecular imaging positive disease, particularly with 1 lesion in his right hip, it’s hard to know whether or not this would take him out of the potential of a therapy that could lead to local control and potentially longterm disease control given that he was to receive systemic therapy with ADT. Many of the patients in the historical studies with radiotherapy or surgery might have had molecular imaging positive disease and we don’t know whether or not some of them could still be cured, particularly if they’re treated with systemic therapy.
We’re entering a new era with the advent of molecular imaging and PSMA [prostate-specific membrane antigen]PET scans have become more widely used. Based upon the imaging information we had in this case, it’s probably reasonable to proceed with definitive therapy, plus systemic therapy.1 Certainly, his progression within a year, with a rising PSA [prostate specific antigen] and new metastases is concerning.
AL-JANADI: I thought based on the STAMPEDE trial [NCT00268476] that it has no value upfront in castration-sensitive prostate cancer management. But now I think it is likely to be of value.
ALUMKAL: I think in the setting of castration-sensitive disease, particularly in the absence of known bone metastases, there’s no role for an osteoclast-targeting agent. Even if he had metastases and was castration-sensitive, we don’t have good data supporting their benefit. In someone with castration-resistant [metastatic] disease to bone, then denosumab [Prolia] or zoledronic acid [Zometa] would be reasonable to reduce skeletal-related events. I think those are reasonable options for him now that he has castration-resistant metastatic disease to bone.


KOKO: If a patient is on ADT, isn’t there a benefit of zoledronic acid at least once a year or denosumab twice a year for bone health?
ALUMKAL: Certainly, in terms of reducing the risk of bone loss, there is a rationale to use these agents. The standard way we use them is for those with mCRPC, those without metastatic disease, or those with castration-sensitive disease. We don’t have good data to suggest that we can prevent skeletal-related events. But there is the potential benefit of reducing osteoporosis.


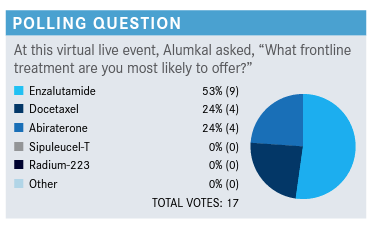
ALUMKAL: Would anyone like to describe what went into their thinking about their choice?
AL-JANADI: The 75-year-old age group perhaps has less data compared with other age groups. So, probably most people would choose the safer oral agent. I thought actually insurance companies require you to use abiraterone [Zytiga] before enzalutamide [Xtandi] because of the difference in price.
ALUMKAL: Yes, I’ve found that to be true depending upon the insurance company and whether or not they mandate abiraterone use before enzalutamide.
AL-JANADI: I’ve read recently that most insurances would require failure of abiraterone before because it is about half of the price of enzalutamide.
R. CHOWDHERY: Most of the time, I haven’t had any insurance issues getting enzalutamide done first. I prefer it just from a tolerability standpoint and not having to commit patients to chronic steroid therapy as well.
A. CHOWDHARY: I think it’s a very fair point for insurance to mandate abiraterone if it is that much cheaper than enzalutamide. I’ve used either as first-line therapy, and never had any pushback. When you look at the data, I’m not sure a lot of people sequence hormonal therapies. I’ve felt like most people don’t believe that sequencing is helpful. I sequence routinely and use abiraterone if I can as first-line and will generally use enzalutamide or apalutamide in a second-, or third-line setting, post-chemotherapy.
ALUMKAL: I think docetaxel [Taxotere] too is certainly a reasonable option in this patient who has a transient response to ADT, has progressed within a year, and has symptomatic disease. Exactly how driven by the androgen receptor [AR] his tumor is remains to be seen. Certainly, using chemotherapy would be a different mode of action.¹
Patients do quite poorly if they progress this quickly after starting ADT. We obviously don’t have randomized data comparing chemotherapy vs an agent like an AR inhibitor in this setting. So, they’re all reasonable options and the patient most likely will end up using several of these therapies.
KYRIAKOPOULOS: [Having] symptoms indicating the presence of visceral disease is a reason to consider more aggressive treatments like docetaxel.
ALUMKAL: Yes. We certainly know that patients with visceral disease who were treated in either the COU-AA-301 study [NCT00638690] or the PREVAIL study [NCT01212991] had worse outcomes and a much shorter duration of tumor control than those who didn’t have visceral disease.2,3 These are patients whose tumors may be less reliant upon the AR and we should think about using chemotherapy earlier vs an AR-targeting agent in them. Certainly, if they have a poor response to initial ADT, I worry more about them being less AR-driven. Perhaps, moving to chemotherapy sooner rather than later is best.
KOKO: Do you take into consideration the length of the duration of response of ADT before switching to chemotherapy?
ALUMKAL: Certainly; one of the things we look at, based upon the SWOG-9346 trial [NCT00002651] data from Dr Maha Hussain, is the 7-month PSA value after starting hormonal therapy.⁴ The lower that number, the better patients tend to do. If it’s less than 0, the average survival is around 6 years; if it’s between 0 and 4, the average survival is around 4 years; if the PSA is greater than 4 after 7 months of starting hormonal therapy, the median overall survival [OS] is around 18 months.
Similar data in terms of outcomes for patients [have] been demonstrated in chemotherapy plus hormonal therapy upfront. Generally, the lower the PSA goes, the better patients tend to do.
For patients whose PSA is increasing very shortly after starting hormonal therapy, I worry about a more aggressive course. Again, we don’t know what the best therapy for these patients are, but I worry more about treating them with another agent that hits the same pathway as medical castration, particularly if they are primary refractory to ADT. I often think about using docetaxel first, rather than going to an AR agent, particularly if they’re symptomatic. Again, we don’t have randomized data to know what’s optimal for these patients. We know if they have an inadequate PSA decline that they’ll do poorly, but we don’t know for certain the best way to treat them. These are patients in whom I think more about using chemotherapy earlier rather than later. If I start them on an oral agent, I follow them fairly closely by checking the PSA in 6 weeks, then 3 months. If there is no benefit then, it may be important to quickly shift over to chemotherapy, which can be quite active in this setting.
I think an option like sipuleucel-T [Provenge] in someone who’s having symptomatic mCRPC wouldn’t be a good option because there aren’t any objective responses. There’s no improvement in progression-free survival [PFS] with sipuleucel-T and there’s no symptomatic benefit. We often reserve radium-223 [Xofigo] for patients, based upon the ALSYMPCA study [NCT00699751] that led to its approval. These are patients who are either unfit for chemotherapy or who have disease that’s already resistant to chemotherapy. For this patient with just 2 bony metastases, radium-223 and sipuleucel-T would probably be at the bottom of my list of options.
PARP inhibitors would be used for patients who have a homologous recombination DNA repair defect and pembrolizumab [Keytruda] for microsatellite instability high [MSI-high] or high tumor mutational burden [TMB] CRPC. Sipuleucel-T is also an option for asymptomatic or minimally symptomatic patients. Platinum-based chemotherapy is an option in patients who have a germline defect or a somatic defect in homologous recombination DNA repair gene.⁵
What other factors besides disease extent would you consider when deciding choice of treatment?
AL-JANADI: This patient had docetaxel stopped because of neuropathy, so it was not progression. I think it's reasonable to consider re-challenge, and start at 60 mg instead of 75 mg/m2.
ALUMKAL: He did progress within 3 months of stopping and had a neuropathy already, which we will assume is ongoing and something to consider in terms of adverse effect [AE] profile for docetaxel. What would steer you towards cabazitaxel [Jevtana]?
KOKO: In this patient, with the presence of peripheral neuropathy, I’ll be reluctant to consider cabazitaxel because it can also be associated with neuropathy.
ALUMKAL: It’s not one of the principal AEs with cabazitaxel, but there is obviously some overlapping toxicity with agents of the same class although the rates are quite lower in cabazitaxel. We worry more about gastrointestinal AEs and neutropenia with cabazitaxel vs docetaxel.
KOKO: I think with the options available, cabazitaxel seems to be the best option for this patient, currently.
ALUMKAL: When deciding on which therapy to use, certainly look at the toxicities that a patient has had so far. Also, what was the benefit with the prior AR-targeting agent or chemotherapy that was used? Patients who are primary refractory to a novel AR-targeting inhibitor are unlikely to benefit from a second AR-targeting agent. Patients who have a more durable control with an AR-targeting agent can benefit from a second AR-targeting agent, particularly if they’re asymptomatic and want to delay chemotherapy. The issues with prescription drug coverage come into consideration too. If someone didn’t tolerate docetaxel and it was not related to an allergy or severe myelotoxicity, cabazitaxel would still be an option if there were other AEs more common with docetaxel than cabazitaxel, including neuropathy.
What are your opinions on the CARD trial [NCT02485691] data? This focused on patients who had a very poor response to an AR targeting agent, a novel AR targeting agent, less than 12 months of disease control, who had also received docetaxel, who randomized to cabazitaxel or a second AR targeting agent. Would anyone like to offer their own personal thoughts about these data?
MATTOUR: It’s what I’ve been doing in practice even before the CARD trial, so it’s just reaffirmed my way of doing it. The data of the OS and the toxicity profile are very compelling.
KARWAL: We know that changing ADT doesn’t seem to make a difference. But there’s data that say cabazitaxel works after docetaxel, so it makes sense.
ALUMKAL: There are subsets of patients who can respond to a second AR-targeting agent, probably in the 20% to 25% range. In patients who had a good response to the first AR-targeting agent, I feel more comfortable using a second one. If the patients have had an inadequate first response to an AR-targeting agent, but they really want to avoid chemotherapy, I think it’s not unreasonable to try a second AR-targeting agent, but counsel the patient that it’s unlikely to work and they’ll probably still need chemotherapy. I think these data would suggest that in a patient who’s had a poor response to a first-line AR-targeting agent and who’s already had docetaxel, cabazitaxel is a superior option to using a second AR-targeting agent.⁶
MATTOUR: Do you factor in the AR-splice variant 7 (V7) status in your decision?
ALUMKAL: The study didn’t stratify for AR-V7 status, so no doubt many of these patients were AR-V7 positive and would not have been predicted to respond to an AR-targeting agent. Some of them could have been AR-V7 negative, and still responded better to cabazitaxel vs a second AR-targeting agent.⁶ I suppose if the AR-V7 was negative, it would give you a greater rationale to try an AR-targeting agent first and have greater comfort doing that. But you could also just prescribe the AR-targeting agent rather than getting the AR-V7 test because in many cases you won’t find circulating tumor cells [CTCs] or it will be AR-V7 positive, in which case you could probably find out the same thing within 6 weeks of enzalutamide or abiraterone therapy.
NEMUNAITIS: I haven’t ordered AR-V7 before, when would you order that?
ALUMKAL: I don’t order it at all because it has no major impact on my decision making in patients who are resistant to an AR-targeting agent. These are patients who have already had docetaxel, for example, with chartered chemotherapy, and then enzalutamide or abiraterone. I think these data would suggest moving forward with cabazitaxel chemotherapy rather than using an AR-targeting agent. Again, in patients who didn’t want to do chemotherapy with cabazitaxel I would probably just try put them in a clinical trial, or try an alternative AR-targeting agent. There hasn’t been widespread adoption of the AR-V7 test even before the CARD study, but with the CARD study, it was a differentiator between who should get a second AR-targeting agent vs chemotherapy. It becomes a moot point because of the improved OS and PFS data with cabazitaxel vs a second AR-targeting agent.
AL-JANADI: In the CARD study, what was the percentage of people who received cabazitaxel post progression if they were randomized to the hormonal arm?
ALUMKAL: I don’t know if they reported [the post randomization crossover] results in that study, and that certainly could have an impact on the OS between the 2 groups. It wouldn’t have an impact on the PFS and the rPFS. But, for these patients, that really is the main treatment option post progression. For someone on cabazitaxel, it would be an AR-targeting agent or radium and, for someone who was treated with the androgen inhibitors, cabazitaxel would be the principal treatment they could receive at progression.
AL-JANADI: If you think that the patient can be counseled for the decision, give them an AR-targeted agent and watch them carefully, if they progress, then switch to cabazitaxel. So, it’s a discussion where you just tell [the patient] what the options are.
ALUMKAL: Yes, I think in the absence of these data, we really didn’t know what to use next. Many of us thought it was probably reasonable to try an AR-targeting agent and delay chemotherapy. But I think, on average, these results would suggest it’s probably preferable in someone who’s had a poor response to an AR-targeting agent, who’s received chemotherapy with docetaxel, to move on to cabazitaxel expeditiously.
NEMUNAITIS: If they have MSI or [a] BRCA mutation, would you use an AR-targeted agent before the cabazitaxel?
ALUMKAL: Yes, I think that would certainly be a shared decision-making discussion in those who have high TMB, or who have MSI. There’s probably a 30% to 50% chance that they could respond to an immune checkpoint inhibitor, so that would be reasonable. Similarly, if they have a homologous recombination DNA repair defect, a PARP inhibitor would be on the table. Based upon the molecular profiling, those could be good options prior to using chemotherapy.
In terms of managing toxicity with cabazitaxel, I commonly use 20 mg/m², based upon the PROSELICA study [NCT01308580] that showed it was not inferior to 25 mg/m² and had less hematologic toxicity. The CARD study used 25 mg/m², but the PROSELICA study would suggest that 20 mg/m² may be better tolerable for patients. In terms of oral vs infusion, obviously it’s a personal decision for patients, whether they want more chemotherapy or not, and whether insurance will cover an oral agent.7
REFERENCES:
1. NCCN. Clinical Practice Guidelines in Oncology. Prostate cancer, version 2.2021. Accessed June 30, 2021.https://bit.ly/3r7khWs
2. Goodman OB Jr, Flaig TW, Molina A, et al. Exploratory analysis of the visceral disease subgroup in a phase III study of abiraterone acetate in metastatic castration-resistant prostate cancer. Prostate Cancer Prostatic Dis. 2014;17(1):34-39. doi:10.1038/pcan.2013.41
3. Alumkal JJ, Chowdhury S, Loriot Y, et al. Effect of visceral disease site on outcomes in patients with metastatic castration-resistant prostate cancer treated with enzalutamide in the PREVAIL trial. Clin Genitourin Cancer. 2017;15(5):610617.e3. doi:10.1016/j.clgc.2017.02.007
4. Hussain M, Goldman B, Tangen C, et al. Prostate-specific antigen progression predicts overall survival in patients with metastatic prostate cancer: data from Southwest Oncology Group Trials 9346 (Intergroup Study 0162) and 9916. J Clin Oncol. 2009;27(15):2450-2456. doi:10.1200/JCO.2008.19.9810
5. Lowrance WT, Breau RH, Chou R, et al. Advanced prostate cancer: AUA/ ASTRO/SUO guideline part I. J Urol. 2021;205(1):14-21. doi:10.1097/ JU.0000000000001375
6. de Wit R, de Bono J, Sternberg CN, et al; CARD Investigators. Cabazitaxel versus abiraterone or enzalutamide in metastatic prostate cancer. N Engl J Med. 2019;381(26):2506-2518. doi:10.1056/NEJMoa1911206
7. Fizazi K, Kramer G, Eymard JC, et al. Quality of life in patients with metastatic prostate cancer following treatment with cabazitaxel versus abiraterone or enzalutamide (CARD): an analysis of a randomised, multicentre, open-label, phase 4 study. Lancet Oncol. 2020;21(11):1513-1525. doi:10.1016/S1470-2045(20)30449-6

















