Morgans Discusses How to Sequence Therapies in Metastatic CRPC
Alicia K. Morgans, MD, MPH, discussed treatment and testing strategies for metastatic castration-resistant prostate cancer.


Alicia K. Morgans, MD, MPH
In a live case-based peer perspectives discussion, Alicia K. Morgans, MD, MPH, associate professor of Medicine (Hematology and Oncology), Northwestern University Feinberg School of Medicine, Chicago, IL, reviewed treatment and testing strategies for metastatic castration-resistant prostate cancer (mCRPC), based a real case of 75-year old patient.


Targeted Oncology™: What are your initial impressions of this case? Do you agree with the treatments used?
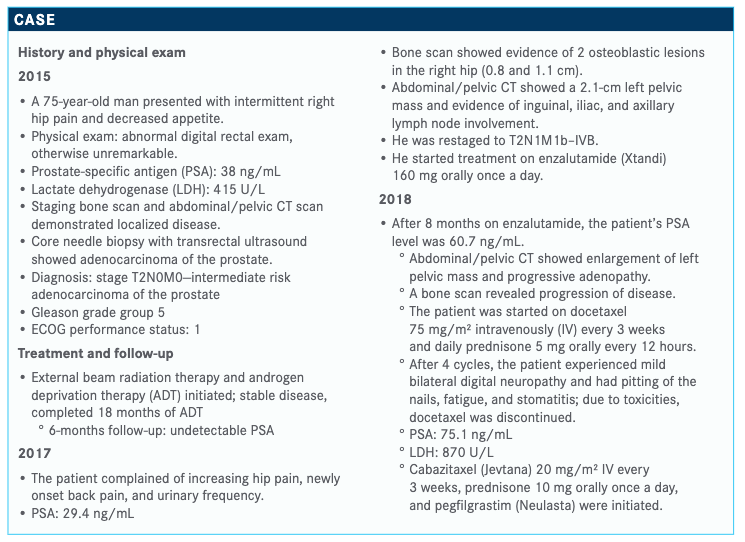
MORGANS: At this point, if we consider this gentleman’s prognosis, we recognize that he received a diagnosis of an initial high-risk localized prostate cancer. Although he was getting his initial therapy that his care team hoped would cure him of his disease, he had progression of disease. He developed meta-static castrate-resistant prostate cancer [CRPC] while on initial androgen deprivation therapy, which is a poor prognostic sign. His second sign of poor prognosis was that, in terms of disease control, he lasted only about 8 months on enzalutamide.
Enzalutamide in the first-line setting for metastatic CRPC can typically last—or we hope will last—at least 12 months and ometimes a little longer. For this patient, disease control was maintained for only 8 months. Those are 2 signs that this patient had an aggressive disease, and we know it’s already metastatic, making his prognosis poor and making it important for us to find a highly effective therapy that uses a different mechanism of action than an androgen receptor [AR]–directed therapy to get the disease down and allow him to maintain quality of life and disease control.
Would you order biomarker testing for this patient? If so, which would you order?
It’s important to consider in metastatic prostate cancer that biomarkers are a critical aspect of our treatment decision making. Biomarkers can include things like DNA-repair defect markers, and this is important in any patient with metastatic disease. We would determine this with germline genetic testing and somatic genomic testing of the tumor tissue. Both are important in understanding whether there may be a targetable DNA-repair defect mutation. We would target these mutations with things like PARP inhibitors. In the third-line metastatic CRPC setting, it might be a good opportunity to use this treatment.
When we think about other biomarkers [such as] AR-V7 [andro-gen receptor variant 7], I wouldn’t necessarily use that marker in this patient, because we already know that he has been exposed to enzalutamide and likely has a cancer that’s resistant to an AR-directed therapy. Having a test showing that he did or did not have the expression of AR-V7 wouldn’t necessarily change my decision process about giving him another AR-directed therapy. I wouldn’t do it because I already know that he has developed resistance and developed it in a relatively short [time].
That’s not a test I would order, but I would order genetic testing and genomic testing to make sure I understood if this patient had a DNA-repair defect that can be targeted. When this patient was tested for DNA-repair defects, he did not have anything in his germline or tumor tissue that was targetable with a PARP inhibitor.
How do you decide on treatment for the patient population with progressive disease?
When deciding on treatment for patients with metastatic CRPC after progression on an AR-directed therapy, I consider whether he disease is symptomatic or asymptomatic. We could consider using sipuleucel-T [Provenge] in patients who have a low burden of metastatic disease and are completely asymptomatic. We are also thinking about whether patients have liver metastases, because we did not test sipuleucel-T in the phase III trial that led to its approval in patients with liver metastases.1
With this patient, we know that he has had some symptoms and a high PSA at the time of his recurrence. Usually, we think about things like sipuleucel-T in patients who do not have any pain or are relatively asymptomatic and also have a relatively low PSA. Those are the patients in whom we think it will work best.
What factors and other therapy options should be considered for this patient?
I would think about other exposures. This patient received chemo-therapy, and so in the setting of exposure to an AR-directed therapy and chemotherapy, I would want to change the mecha-nism of action away from an AR-directed therapy and focus on things like PARP inhibitors if the patient had DNA-repair defect; another chemotherapy if the patient did not have that defect; or, potentially, radium, which could be an option in patients who have only bone metastases, no lymph node metastases, and no visceral disease.
For this patient, we know he started with lymph node meta-static disease, so radium would not be expected to maintain disease control because it does not affect any disease outside the bone. Chemotherapy would be my choice [for him]. Even though he’s had progression on docetaxel chemotherapy, we know that switching to cabazitaxel [Jevtana] chemother-apy can be highly effective both in terms of pain control and prolonging life.
Why do patients benefit from the use of cabazitaxel? Please discuss the trial that showed these benefits.
When I think about tolerance to chemotherapy, particularly the tolerance of cabazitaxel, I think about some studies that were done for cabazitaxel that demonstrated that at the 20 mg/m2 dose, [patients] had less fatigue and less neuropathy than docetaxel at a standard dose of 75 mg/m2. Cabazitaxel in my clinic and in those trials is quite well tolerated, even in older patients.2
We could consider using sipuleucel-T in patients who have low burden of metastatic disease and are completely asymptomatic. We are also thinking about whether patients have liver metastases, because we did not test sipuleucel-T in the phase III trial that led to its approval in patients with liver metastases.”
What we saw in the CARD trial [NCT02485691] was that cabazitaxel was better tolerated than a second-line AR-targeted agent in patients who had already had progression on AR-targeted agent and at least 1 line of chemotherapy.3 For those patients, there was a longer time to pain progression, and they had a better pain response than patients treated with a second AR-targeted agent. These patients felt better than those on what we normally consider to be tolerable treatments. Even in older patients or in patients who have pain, cabazitaxel chemotherapy can be well tolerated with relatively low neuropathy and fatigue compared with other chemotherapy agents, and we would want to [help] these patients with our supportive measures. We can get them through it, and they seem to tolerate it well.
What was the design of the CARD trial?
In the CARD trial, patients who had metastatic CRPC and had progressed on 1 AR-targeted agent and docetaxel chemotherapy were randomized to receive treatment with the other AR-directed therapy or cabazitaxel at its standard dose, 25 mg/m2, plus pegfilgrastim. Patients were followed for radiographic progres-sion-free survival [PFS] and overall survival [OS] in this trial.
Describe the efficacy and the toxicity profile of this trial.We found that patients had prolonged PFS and OS in the CARD trial.
Importantly, the CTCAE [Common Terminology Criteria for Adverse Events]–graded events, which tell us about the toxicity of the agents, suggested that the chemotherapy did not have any adverse effects [AEs] outside its traditionally considered AE profile. There were more grade 5 AEs leading to death in the arm of patients who were treated with the AR-targeted therapy and fewer grade 5 events in those who received chemotherapy.
These patients had a better pain response when they were treated with chemotherapy, probably because of better disease control. We saw that this was what I consider a practice-changing study in that it defined for us a path forward in the third-line setting in metastatic CRPC, where we had not had trials that told us what happens to patients who already received first- and second-line treatments for patients with metastatic CRPC.
Patients seemed to tolerate the treatment well—as I said, both in terms of CTCAE and patient-reported outcomes—with their overall quality of life also reported to be better when they were treated with cabazitaxel compared with the AR-directed therapies at the 3-month assessment by the overall quality-of-life measure, FACT-P [Functional Assessment of Cancer Therapy-Prostate]. The drug was well tolerated and ultimately improved survival in this heavily pretreated third-line metastatic CRPC population.
Do any data support the use of sequential AR-targeted therapies in this setting?
When I think about using a second AR-targeted agent after exposure to and progression on a prior AR-targeted agent in the metastatic CRPC setting, I talk to patients about the inadequacy of that therapy, sequencing, and my expectation that the treatment probably will not help them. This has been demonstrated in the control arm of the CARD trial, but it has also been demonstrated in other settings.
For example, in the phase III PROfound trial [NCT02987543] that looked at men with metastatic CRPC who had DNA-repair defects, men were randomized to treatment with olapa-rib [Lynparza] or the other AR-targeted agent [enzalutamide or abiraterone (Zytiga)]. This was in patients who had already progressed on chemotherapy and an initial AR-targeted agent. We saw that the radiographic PFS of that control arm, the second AR-targeted agent, was about 3.5 months, which is similar to what we saw in the CARD trial.4
We are consistently seeing in patients who have already progressed on an initial AR-targeted agent—whether they progress within 12 months, as they did in the CARD trial, or whether they simply progress at any time point, which they did in the PROfound trial—that the expected time to controlling disease and preventing radiographic progression is short.3,4 And the reason it’s probably around a 3-month time point is because that is when they were doing the radiographic assessment. Most of these patients are progressing on the first or the second radiographic assessment, suggesting that we’re not controlling the disease growth.
There are a few patients who may respond to a second AR-targeted agent. Usually I think about use of enzalutamide after abiraterone being potentially more effective, but this is not my first choice, and it’s something I highly recommend patients consider
Case-Based Peer Perspectives Spotlight 55Case-Based Peer Perspectives Spotlight 55not doing, because we know that the mechanisms of resistance are similar. Especially in settings where we have an aggressive cancer and need to control the disease, doing this is not expected and could waste time for patients, leading to decline in functional status, potentially closing the door for them to get something like chemotherapy, which may prolong their life. But this has to be given in patients who are well enough to tolerate it.
How do you decide on sequencing for the available regimens in this setting?
When I think about treating patients with metastatic CRPC, I think about all the agents we have at our disposal, and there are many. The most important thing to me, when I’m thinking through their next treatment, is understanding what they had in the past and how we can use a diff erent mechanism of action for their next line of treatment to sequence one therapy after another—hopefully, prolonging time and quality of life multiple times over by sequencing available treatment options that patients have over time. For example, if a patient has had an AR-targeted agent and docetaxel chemotherapy, the things I think about next will be something with a new mechanism of action or something that has demonstrated that after those 2 agents, it can still be eff ec-tive in terms of prolonging life and making patients feel better.
The option could be, in an asymptomatic patient, sipuleucel-T, although if this is a heavily pretreated population, most patients seem to benefit with sipuleucel-T. For cabazitaxel chemotherapy, we now have the CARD data to show that we can certainly sequence it and, in the third-line setting, prolong life and improve quality of life. Or perhaps we could use radium in patients who have only bone metastases and no lymph node metastases or visceral metastases.
I also always think about sequencing a patient’s DNA and the tumor DNA to understand whether there are genetic germline mutations that may be targetable or somatic genomic mutations in the tumor tissue. We can use PARP inhibitors to potentially target these DNA-repair defect mutations that make patients sensitive to these drugs.
Would you use regimens that are being examined in clinical trials?
I [will] think about clinical trials and expanding the options for patients by giving them something that’s not yet FDA approved. There are multiple things, whether they’re radiopharmaceuti-cals, AR-degrading agents, or other combinations that may be eff ective that we’re just starting to understand. These options are available only through clinical trials, so that is always some-thing I think about, as well.
The landscape of treatment for patients with metastatic CRPC is changing rapidly and dramatically, with options demonstrating efficacy in both prolonging OS and maintaining quality of life. This includes treatments we’ve already had approved, such as cabazi-taxel, as well as things on the horizon, like PARP inhibitors.5 It also includes things that are still to come, such as radiopharmaceuticals or other agents—whether they are vaccines, AR degraders, or other approaches that are new for our patients.
There are so many options that it’s important for us to consider what patients have had before and think about changing the mechanism of action, or using treatments that we know can be effective after exposure to these other agents, to get the best results for our patients and not waste time with things that we think have a low likelihood of working. Because when we waste time, it’s not only the potential for other treatments that we waste but patients’ quality of life suffers, as well. The landscape is changing. There are many opportunities, and it’s an exciting time to be a treating physician for men with metastatic CRPC.
References:
1. Provenge. Prescribing information. Dendreon Pharmaceuticals LLC; 2017. Accessed April 24, 2020. provenge.com/Portals/_default/skins/provengedtc/downloads/PRV.0039.USA.18-%20Provenge%20Prescribing%20Information.pdf
2. Oudard S, Fizazi K, Sengeløv L, et al. Cabazitaxel versus docetaxel as fi rst-line therapy for patients with metastatic castration-resistant prostate cancer: a randomized phase III trial-FIRSTANA. J Clin Oncol. 2017;35(28):3189-3197. doi:10.1200/JCO.2016.72.10683.
3. de Wit R, de Bono J, Sternberg CN, et al; CARD Investigators. Cabazitaxel versus abiraterone or enzalutamide in metastatic prostate cancer. N Engl J Med. 2019;381(26):2506-2518. doi:10.1056/NEJMoa1911206
4. Sandhu SK, Hussain M, Mateo J, et al. PROfound: phase 3 study of olaparib versus enzalutamide or abiraterone for metastatic castration-resistant prostate cancer (mCRPC) with homologous recombination repair (HRR) gene alterations. Ann Oncol. 2019;30(suppl 9):ix188-ix189. doi:10.1093/annonc/mdz446.0075.
5. FDA approves lower dose of cabazitaxel for prostate cancer. FDA. Published September 14, 2017. Accessed April 23, 2020. fda.gov/drugs/resources-information-approved-drugs/fda-approves-lower-dose-cabazitaxel-prostate-cancer



















Survivorship Care Promotes Evidence-Based Approaches for Quality of Life and Beyond
March 21st 2025Frank J. Penedo, PhD, explains the challenges of survivorship care for patients with cancer and how he implements programs to support patients’ emotional, physical, and practical needs.
Read More




