Matous Evaluates Treatment Strategies for Transplant-Ineligible Multiple Myeloma
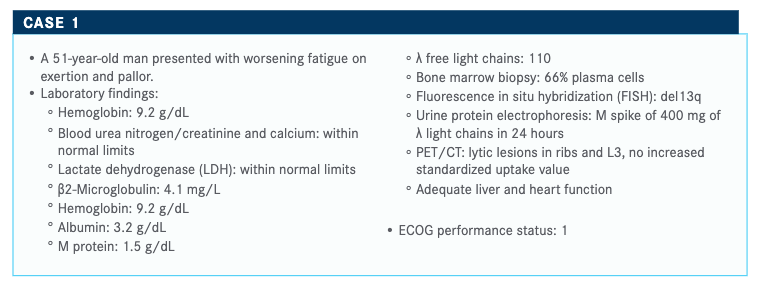
Jeffrey Matous, MD, discussed strategies for treating a 51-year-old male patients with transplant-ineligible multiple myeloma, during a live Targeted Oncology case-based peer perspectives conversation with other experts.



Jeffrey Matous, MD, medical director of Colorado Blood Cancer Institute in Denver, CO discussed strategies for treating a 51-year-old male patients with transplant-ineligible multiple myeloma, during a live Targeted Oncology case-based peer perspectives conversation with other experts.


Targeted Oncology™: How do you discuss prognosis with your patients?
MATOUS: I tell my patients I’m going to treat with curative intent. I think it’s a great way to tell them that we’re going to treat. Patients want to be hopeful. The goal of treatment is longer survival with excellent quality of life.
What is the age cutoff for transplant-eligible patients in this setting?
In Europe, the cutoff has been 65 years of age, but in the United States, that has been long abandoned. When discussing transplantation, it’s more of a physiological definition than a chronological definition for who is eligible.
How do you define fit patients at your institution? What questions do you normally ask to find out?
It takes me about 3 seconds to assess the patient’s fitness when I walk into the examination room. You can tell their level of activity, and you can ask the patient what they do for exercise. And if they reply with “I skied 60 days last winter,” then you know their fitness.
Do you refer to the National Comprehensive Cancer Network (NCCN) myeloma guidelines1?
Occasionally. Interestingly, the guidelines contain just 1 regimen that is a quadruplet treatment, which is daratumumab [Darzalex]–VTd [bortezomib (Velcade)/ thalidomide (Thalomid)/dexamethasone]. VTD was the standard for a few years, but adding daratumumab-VTd is the result of the Cassiopeia trial [NCT02541383].2
What are the role of and timing for the use of stem cell transplant in newly diagnosed multiple myeloma?
Four studies looked at stem cell transplant in the patient with newly diagnosed multiple myeloma: IFM 2009 [NCT01191060], FORTE [NCT02203643], Cassiopeia, GRIFFIN [NCT02874742].
IFM 2009 was published in the New England Journal of Medicine, and it looked at up-front transplant versus delayed transplant.. The FORTE trial is an important trial out of Italy.⁴ This trial looks at up-front KRd [carfilzomib (Kyprolis), lenalidomide (Revlimid), dexamethasone] versus KCd [carfilzomib, cyclophosphamide, dexamethasone] with a transplant arm. Cassiopeia is a trial that resulted in the approval of daratumumab-VTd.⁵ GRIFFIN is still early on, with fewer patients than Cassopeia.⁶ GRIFFIN is a trial that we’re keeping an eye on. Patients in the consolidation maintenance phase are still being followed. Across these 4 trials, we’re seeing high postconsolidation VGPR [very good partial response] rates in these patients.
IFM 2009 evaluated patients who were 65 years of age or younger who were treatment na.ve and asymptomatic. The trial involved 3 cycles of RVd, after which stem cells were collected. After the patients were randomized, treatment with 6 more cycles of RVd followed versus stem cell transplant. All arms received lenalidomide maintenance therapy. For patients in the RVd-delayed transplant arm who progressed, undergoing transplant was recommended.
What are the significant findings from the FORTE study?
In FORTE, a 3-arm trial, patients were randomized to either 4 cycles of KCd, 4 cycles of KRd, or 4 cycles of KrD. After induction, patients who received KCd and 1 arm of patients who received KRd underwent allogeneic stem cell transplant. The patients in the remaining KRd arm continued with 8 more cycles of KRd, for a total of 12 cycles of KRd [KRd12].
This is followed by a second randomization between KR and lenalidomide. None of the maintenance data have been reviewed at medical conferences at this point. Currently, response data are available, including MRD [minimal residual disease]. What I’m curious about is if we should be inducing with KRd or RVd. This study does not address that question, but I think SWOG evaluated this, and findings are expected to be presented during ASCO [American Society of Clinical Oncology Annual Meeting].
SWOG looked at up-front KRd versus RVd in the nontransplant setting. ASCO will have an uncharacteristically heavy myeloma session, with practice-changing data likely to be reported.
Getting back to FORTE, if we review the stringent CR [complete response; sCR], CR, and MRD-negative data, for KRd versus transplant plus KRd, all these responses are close together, and there appears to be no difference in the findings.
This suggests that both these treatment modalities offer similar benefit. These data are not mature yet, but it appears that for patients who received transplant plus KRd, the early relapse rate is lower, 8% versus 17% in the KRd arm, which is observed in the higher-risk group. Reviewing multivariate regression, the risk of early progression is reduced in the transplant arm versus the KRd12 arm. For patients who relapsed in the nontransplant arm, it’s presumed that they underwent transplant. Either arm suggests that you can delay relapse through transplant.
Cassiopeia evaluated a quadruplet regimen versus a triplet regimen. What was significant in this trial?
[With] Cassiopeia, it appears, based on the sheer number of patients, like a breast cancer trial with its 1085 patients. This European study enrolled garden-variety, standard-risk, younger patients with myeloma. These patients were randomized to receive VTd or daratumumab-VTd. Stem cells were harvested and transplanted for both arms, followed by consolidation. Patients underwent 6 cycles of either the triplet or quadruplet regimen and then had a second randomization. At the second randomization, patients were either observed with no maintenance therapy or received daratumumab maintenance.
The primary end point of sCR was met, with patients in the daratumumab-VTd arm reporting an sCR of 29% and patients in the VTd arm reporting an sCR of 20%. What’s interesting in this trial is that sCR favored the quadruplet regimen except for patients at high risk. Similarly, MRD-negative status favored the quadruplet arm reported at 64% versus the triplet arm, reported at 44%.
Please discuss important data from GRIFFIN.
This trial is going to be a practice changer. It looked at newly diagnosed, transplant-eligible patients up to 70 years of age. Inclusion criteria to enroll was reasonable renal function. The trial evaluates daratumumab—RVd versus RVd—the induction phase if 4 cycles of each, then stem cell collection, followed by 2 cycles of consolidation with patients on the same regimen. It’s interesting to note that 90% of patients on the quadruplet regimen get transplanted, and 76% of patients in the triplet get transplanted, and this is due to progression.
For GRIFFIN, the initial data were just from a safety run-in that involved 16 patients. And yet, in these patients, VGPR is high after transplant. The sCR is 25%, CR is 38%, and VGPR is 38%. Everyone responded. During maintenance, a deepening response was observed. This allowed the trial to go forward to phase III.
The sCR by the end of consolidation was 42.4% in the daratumumab-RVd arm versus 32.0% in the RVd arm. That’s a decent sCR rate after therapy with daratumumab-RVd. The other thing we have learned again and again in myeloma is that responses deepened over time. Response rates and depths were greater for daratumumab-RVd at all time points.
Will MRD be a factor in the FDA’s decision to approve a treatment moving forward?
Currently, the FDA bases its approval on progression-free survival [PFS]. I think the FDA is going to be more open to MRD. In the GRIFFIN trial, the MRD negativity rate at data cutoff for the quadruplet therapy arm was 51.0% compared with 20.4% in the triplet therapy arm.6
How do you measure MRD rate?
MRD rate is growing in importance, so it is important to obtain accurate readings. In fact, more studies are looking at the MRD rate but also noting if MRD is sustained over time or not. That will be critical.
The easiest way to obtain an MRD rate is to use high-quality, at least 8-color flow cytometry—the standard is EuroFlow because it’s readily available—and next-generation sequencing [NGS]. Good flow cytometry is 10-5, and good sequencing depends on how many cells you are sequencing. If you are sequencing enough cells, then attaining a 10-6 [concentration] is obtainable.
If you attend a lecture and an investigator is talking about MRD, the question you need to ask is “What was your technique?”
How did the quadruplet regimen compare with the triplet regimen for sCR and MRD in GRIFFIN?
What was demonstrated in GRIFFIN was that for MRD, the quadruplet therapy was favored over the triplet therapy. D-RVd was favored across all subgroups for MRD negativity and across all subgroups for sCR rate, except high-risk cytogenetics and ISS [International Staging System] stage III disease. I emailed Peter Voorhees, MD, about this, and he said that the numbers got really small for high-risk disease. He had 100 patients, and basically 15% of patients are usually high risk.
How should clinicians address the neuropathy that is usually associated with bortezomib for this patient population? What do you tell your patients when they are about to go on this drug?
We see a significant number of patients develop neuropathy, most likely attributed to bortezomib. I’ll mention that the way our nurses ask about neuropathy is important. If they ask “Do you have neuropathy?” the patient will respond “No,” because they fear that if they say yes, you will stop their treatment.
However, if we ask if patients have numbness or tingling or lightning bolts of pain in there, we’re going to get more positive answers. It’s better to explain to patients that we can attenuate their dose of bortezomib so that they are treated longer and more effectively. We’re still seeing a lot of patients referred to us for transplant on RVd coming in with grade 2 neuropathies with pain. We have to do better than that.
The first thing I do when considering neuropathy is tell the patient to be paranoid about neuropathy. That’s the terminology I use. Be paranoid about neuropathy and report anything more than mild numbness or tingling. If I see that, I immediately hold the bortezomib. I hold it until the adverse effects dissipate down to grade 1 or less. Then I will consider reinstituting the drug with a dose modification, either by decreasing the dose or going to weekly dosing or both.
References:
1. National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology. Multiple myeloma (version 3.2020). Accessed April 24, 2020. https://bit.ly/352Twrb
2. Moreau P, Attal M, Hulin C, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): a randomised, open-label, phase 3 study. Lancet. 2019;394(10192):29-38. doi:10.1016/S0140-6736(19)31240-1
3. Attal M, Lauwers-Cances V, Hulin C, et al; IFM 2009 Study. Lenalidomide, bortezomib, and dexamethasone with transplantation for myeloma. N Engl J Med. 2017;376(14):1311-1320. doi:10.1056/NEJMoa1611750
4. Gay F, Cerrato C, Petrucci MT, et al. Efficacy of carfilzomib lenalidomide dexamethasone (KRd) with or without transplantation in newly diagnosed myeloma according to risk status: results from the FORTE trial. J Clin Oncol. 2019;37(suppl 15; abstr 8002). doi: 10.1200/JCO.2019.37.15_suppl.8002
5. Moreau P, Attal M, Hulin C, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): a randomised, open-label, phase 3 study. Lancet. 2019;394(10192):29-38. doi:10.1016/S0140-6736(19)312401.Published correction appears in Lancet. Published online June 14, 2019. doi:10.1016/S0140-6736(19)31403-5
6. Voorhees PM, Kaufman JL, Laubach JP, et al. Daratumumab, lenalidomide, bortezomib, & dexamethasone for transplant-eligible newly diagnosed multiple myeloma: GRIFFIN. Blood. Published online April 23, 2020. doi:10.1182/blood.2020005288.














Gasparetto Explains Rationale for Quadruplet Front Line in Transplant-Ineligible Myeloma
February 22nd 2025In a Community Case Forum in partnership with the North Carolina Oncology Association, Cristina Gasparetto, MD, discussed the CEPHEUS, IMROZ, and BENEFIT trials of treatment for transplant-ineligible newly diagnosed multiple myeloma.
Read More

