Roundtable Discussion: Voss Looks at Integrating New Approaches in Clear Cell RCC Treatment
During a Targeted Oncology™ Case-Based Roundtable™ event, Martin H. Voss, MD, discussed with participants their goals and approaches when considering third-line therapy for patients with advanced clear cell renal cell carcinoma.


Martin H. Voss, MD (Moderator)
Clinical Director
Genitourinary Medical Oncology Service
Memorial Sloan Kettering Cancer Center
New York, NY



CASE SUMMARY
- A 54-year-old man with a history of metastatic renal cell carcinoma (RCC) had undergone a left nephrectomy and adrenalectomy. He had clear cell RCC and metastases in his adrenal gland. Four years later, the patient had a recurrence of cancer, and a biopsy showed lung nodules consistent with clear cell RCC. In retrospect, it had been present on scans for at least 2 years prior to biopsy.
- The patient was observed based on the low volume and indolence of the disease and the patient’s preference. Eighteen months later, reexamination showed continued indolent growth on scans, with an increased total tumor burden and a new paratracheal lymph node (2.0 × 1.5 cm). A decision was made to initiate systemic therapy with pembrolizumab (Keytruda) plus axitinib (Inlyta).
VOSS: Do you all generally pull up the National Comprehensive Cancer Network [NCCN] guidelines1 for any [patient with kidney cancer] that you see? Is it something that you only go to in a tricky case? To what extent do you use the panel recommendation?
RAI: I think only in a tricky case. I find that the NCCN guidelines a lot of times are useful to get things approved from insurance. If it’s in the NCCN guidelines, then it’s easy to quote that and get it approved.
VOSS: It’s something you can cite in the process of approval, yes. Has anyone else had that experience? Do you use the NCCN recommendations commonly for peer to peer?
SOTIRESCU: Yes, I’m using the recommendations as a kind of bible for updating. You can now have a clear picture in 2 seconds when you have to make a life-changing decision. We are so busy in the practice, and I find the NCCN recommendations amazingly helpful from all points of view. I’m using [them to know the recommendations’] categories. I’m also using the columns at the end that are filled with cost effectiveness [and other information]. There are a lot of things you can use the NCCN recommendations for nowadays. [For me, they are] extremely influential.
CASE UPDATE
- When the patient returned for follow-up, the disease was stable. Adverse events reported were moderate diarrhea, well controlled with antidiarrheal medication, and mild fatigue. After cycle 6, the patient developed fatigue, mild shortness of breath, and mild cough without chest pain. The pulse oximeter reading was 93% at rest. He had no fever and no recent sick contact, and his influenza vaccination was up to date. Infectious work-up was negative.
- After approximately 18 weeks, a chest CT confirmed grade 3 pneumonitis. Pembrolizumab treatment was held, and intravenous steroids were administered. Pembrolizumab was discontinued, and the patient continued axitinib.
- Fourteen months after initiation of systemic therapy, the patient reported increasing back pain, mild nausea, weight loss, and new onset of persistent rib pain. Imaging confirmed disease progression:
- The paratracheal lymph node had been 2.0 × 1.5 cm previously and was now 2.5 × 2.8 cm.
- There were new mediastinal and hilar nodal involvement, new retroperitoneal lymph nodes, and new lytic lesions.
- ECOG performance status: 1
- Cabozantinib (Cabometyx) 60 mg once a day was initiated, but 4 months later, disease progression was documented. The patient wanted to continue active therapy.
VOSS: This patient progressed on axitinib plus pembrolizumab and went on to receive second-line cabozantinib at the full dose (60 mg) and unfortunately did not have great benefit from it. The first interim scan 4 months later documented disease progression. The patient, however, tells you they’re still motivated to continue systemic therapy.
DISCUSSION QUESTIONS
- What are the goals of therapy going into the third line?
- What factors influence your third-line regimen selection for a patient such as this?
VOSS: Now we are heading into the third line in someone [with disease that] is behaving quite aggressively. Primary disease progression on second-line therapy has been seen. I’m curious to hear how your consideration is different, going from second to third line vs from first to second line. Specifically, in a patient who’s more heavily pretreated and where second-line therapy has fared in a certain way, what are the things that go into decision-making for you? Is this the exact same approach you choose when figuring out second-line therapy? Do you think about other factors?
EFIOM-EKAHA: Similarly to frontline and second-line treatment decision-making, you’ll be looking at what the patient received and progressed on and the tolerability, but maybe more important here is that short duration of benefit from second-line therapy. Obviously, that was not good. I think that in a fit and motivated patient, I’d be looking for a clinical trial because, quite honestly, the data with currently available third-line treatment are not that encouraging. A clinical trial would be [my choice] up front, especially in a motivated patient.
VOSS: Is your consideration of a clinical trial for this patient based on the number of lines of therapy, or is it based on his lack of response to second-line therapy?
EFIOM-EKAHA: Both. In terms of not having excellent third-line options, [I will say that] tivozanib [Fotivda] is, in my opinion, not a grand slam. But with his tempo of disease and progressing so rapidly even with second-line therapy, it is hard to imagine he’d be getting anything fantastic with my third-line treatment. So it’s more [a question of] whether there is anything else that I can offer that has a chance of doing better than what I think tivozanib would do.
VOSS: Understood. Now I’m curious to hear risk categories listed here. Technically, the NCCN group has demonstrated that risk assessment can be done at the first line, second line, and third line using their model.1 I’m curious. Is anyone here calculating International Metastatic RCC Database Consortium risk in heavily pretreated patients, like a patient heading into third-line therapy? I’m not trying to put you on the spot. There’s no right or wrong answer. I’m just curious if anyone does this routinely, if it helps you make decisions, or if you only do it at the first line because that’s where most of the data are. Is this common practice for you?
COSTELLO: To my knowledge, in the first-line setting there’s clearly a decision tree that’s based upon what scoring is done and favorable characteristics vs unfavorable characteristics. The treatment paradigm is a little different. As you move into second-line therapy and beyond, I’m unclear [as to whether] any data suggest that I should treat differently based upon that scoring system, so I don’t routinely redo it.
VOSS: I would agree that there are no strong data to guide us. Although if you look at trials in the second- and third-line setting, you will get the breakdown of patients based on their risk status. It’s not a data-free zone, but you are right—the NCCN for good reason does not break down their recommendation [in terms of scoring].
Are there specific regimens that you’re more inclined to use in the third line for patients who have had a rough time with toxicities previously?
QIN: I haven’t treated enough patients yet, but I did have a patient [for whom we used] 4 different lines [of therapy]. By the end of the treatment, he just couldn’t tolerate it. For me, as a new graduate, I think [as part of] my principle to treat patients and [help them] live longer and feel better, I always talk about tolerability and the toxicities. My mentors say they see it as a choice. So I always talk to the patient about what their goal is and choose the [therapy] that they can tolerate.
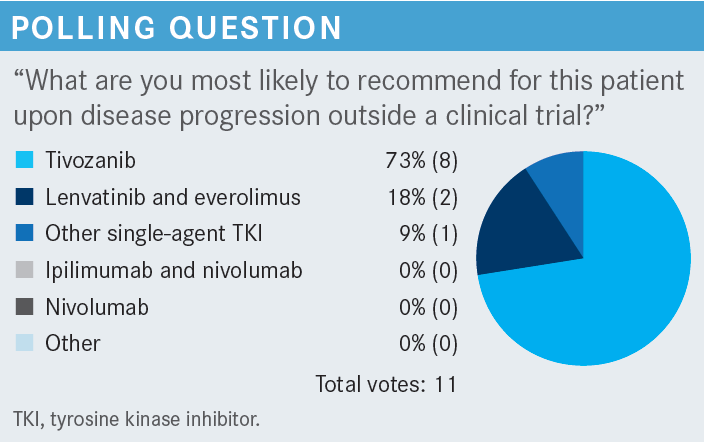
VOSS: Do you have a go-to drug for patients who have a rough time? Is there a drug you’re more drawn to if patients have lots of toxicity? [For example,] the various single-agent tyrosine kinase inhibitors [TKIs]? This patient had axitinib and cabozantinib, so now you could go on to tivozanib or you could try to do lenvatinib [Lenvima] plus everolimus [Afinitor].
You could do any of the other TKIs such as pazopanib [Votrient], sunitinib [Sutent], and so forth, but is there something specific that anyone likes in this setting, or is it sort of a free-for-all? Again, there is no right or wrong answer here. I’m just trying to figure out how you all practice.
RAI: I think it depends on what you’ve used on previous lines. If you used a checkpoint inhibitor on the first line, then maybe you went to a TKI. Maybe they didn’t have a lot of disease and had slow progression, so you did a single-agent TKI, and then in the third line, maybe you want to combine [that with] everolimus (Afinitor).


DISCUSSION QUESTIONS
- With respect to the data from the TIVO-3 study (NCT02627963), is there anything that you were not aware of that strikes you as relevant for patient decision-making?
- What toxicities are most concerning to you in this setting? Which do you find most challenging to manage?
VOSS: Does anyone want to comment on the TIVO-3 data and how you proceed? Maybe I’ll let Dr Loaiza-Bonilla comment. What are your thoughts upon seeing the data, the comparison between tivozanib and sorafenib [Nexavar] in the phase 3 study?
LOAIZA-BONILLA: The standard-of-care arm is no longer relevant, but still I found interesting the fact that patients who had received prior immuno-oncology and TKI therapy still responded [From the Data2].


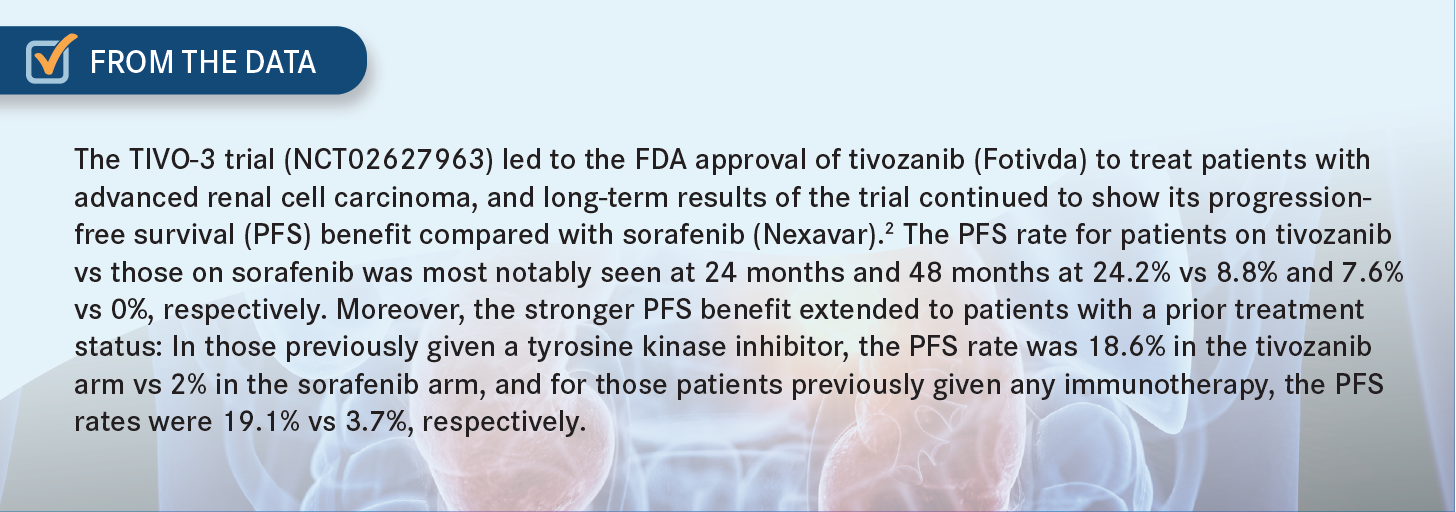
Typically, patients who had been receiving other treatment options, even when using a broader TKI, would not have the responses that we see [reflected in these data], so I think [this study is] relevant. This is not a drug that I have used in the past, but it makes me interested to try it out in some of my patients and see how they do in terms of safety profile and responses.
VOSS: [Let’s consider the] pivotal studies that led to the approval of each of these drugs [tivozanib, cabozantinib, axitinib, lenvatinib (Lenvima), everolimus, and sorafenib] and [compare] any-grade and high-grade toxicities for class-specific TKI adverse events.3-8 All of these drugs bring about a fairly high amount of hypertension. What stands out, certainly, is the lenvatinib plus everolimus combination.
As you might expect, [these] 2 drugs with overlapping toxicity profiles caused quite a bit of fatigue [of all grades, in 73% of patients; of grades 3 and 4, in 18% of patients]. Some of these agents, specifically the more target-specific ones, cause less toxicity than others. Compare [the diarrhea caused by tivozanib all grades, 33%; grades 3 and 4, 2%]3 with that of lenvatinib plus everolimus [all grades, 81%; grades 3 and 4, 19%].6,7
If you look through these [data and] think about your own practice, is there something that stands out as the toxicity that you find most challenging in later-line patients like this, something that is specifically difficult in more heavily pretreated patients rather than a patient who is in the first line?
COSTELLO: Fatigue is one that is a real challenge in this setting. These patients are often a lot more beaten up, both from [the] disease and from prior therapy. Getting through a course of everyday life is a lot more challenging for them. I haven’t used tivozanib, but with a lot of the other drugs, I’d argue the fatigue in the third-line setting is probably worse than is represented here [in these data].
VOSS: In the real world?
COSTELLO: Yes.
VOSS: How do others feel about that? Any other toxicities that you find challenging?
BARSOUK: Diarrhea is quite significant in the third line and significantly affects the patient’s quality of life. It’s present in all different treatment options, particularly when you combine lenvatinib and everolimus, [which together produce diarrhea at] quite high rates. This could be on top of fatigue and asthenia.
This could be a limiting toxicity, requiring dose adjustments and even holding the dose and discontinuation if necessary. But in the third-line setting, when we really emphasize the patient’s quality of life, this [toxicity] could significantly affect it, not only having diarrhea, but [subsequent] dehydration, electrolyte imbalance, and the need for replacement and intravenous fluids. All this, I think, is significant.
JI: I was wondering, practically, how a particular [adverse] effect can be managed. Like for hypertension, for a patient who’s not on blood pressure medication, does 5 mg daily of amlodipine [Norvasc] take care of it, or is it difficult to manage? In the same way, diarrhea: Can some loperamide [Imodium] take care of it, or [at some] point do we have to dose reduce or even discontinue? I think that kind of information would be most relevant, especially in later lines.
VOSS: Regarding the clinical trials, generally the way these protocols are written is you start with supportive medications for low-grade toxicities. If the patient presents up front with a high-grade event, the protocol may ask you—force you— to dose reduce.
If you have a patient who comes in with grade 3 or grade 4 diarrhea on a clinical trial, of course we’re going to give them loperamide, but often you are forced to go down on the dose. The dose adjustments are quite frequent on some of these trials.
DISCUSSION QUESTIONS
- What is your preferred subsequent-line sequencing strategy after each of the following first-line combination regimens?
- Axitinib plus pembrolizumab
- Cabozantinib plus nivolumab (Opdivo)
- Lenvatinib plus pembrolizumab
VOSS: [We have here] 3 different TKI plus I-O [immuno-oncology] options. What if this patient were to start with cabozantinib/nivolumab or with lenvatinib plus pembrolizumab? Would your recommendation for second line differ? How so? Do you have a standard sequence here to consider?
EFIOM-EKAHA: I would say that if cabozantinib wasn’t part of your frontline regimen, that cabozantinib would be my go-to second line. The [combination of] cabo/nivo [cabozantinib plus nivolumab] is a little tricky because now you’ve used cabozantinib. My assumption is the patient was progressing while on cabo/nivo and stayed on the cabozantinib, and then 2 years later they’re progressing. And then I [would] wonder [whether] I could reintroduce immunotherapy. But if they progress on cabo/nivo, and they’re fit and can tolerate it, then I think my option would be to go to lenvatinib plus everolimus.
VOSS: Interesting. What does everyone else think? Dr Kosteva, what are your thoughts? If you had a patient on first-line cabo/nivo, what would you do in the second line?
KOSTEVA: I think if I had [used] cabo/nivo, I might do lenvatinib plus everolimus.
VOSS: Similar to what we have heard then. Does everyone have a favorite sequence in terms of what to use after the other? I think Dr Efiom-Ekaha was clear that he likes cabozantinib. He uses a lot of cabozantinib in the second line, but if patients have had it, then he goes to lenvatinib plus everolimus. Is that how all of you mostly practice? You have your go-to drug, and then you switch things around?
RAI: I think that’s what I do. I try not to use cabozantinib up front. I feel like I can use it as a single agent, so I try to save it. I try to use it maybe in the second line or third line and then maybe use lenvatinib and everolimus.
BARSOUK: That’s the reason you have 2 frontline nivolumab-based regimens, [including] 1 pure combination immunotherapy [nivolumab and ipilimumab (Yervoy)], so I would like to use that in patients with moderate or high risk [and] preserve cabozantinib for the second line.
VOSS: If you use ipilimumab plus nivolumab up front, then cabozantinib would be your second-line regimen of choice?
BARSOUK: Yes.
VOSS: Got it. I have another question. Tivozanib is approved [for use in the] third and fourth line.9 Is anyone using that in the second line, outside of its label?
BARSOUK: I used [it in] 1 patient.
REFERENCES
1. NCCN. Clinical Practice Guidelines in Oncology. Kidney cancer, version 3.2023. Accessed January 17, 2023. https://bit.ly/2TAx1m3
2. Atkins M, Verzoni E, Escudier B, et al. Long-term PFS from TIVO-3: tivozanib (TIVO) versus sorafenib (SOR) in relapsed/refractory (R/R) advanced RCC. J Clin Oncol. 2022;40(suppl 6):362. doi:10.1200/JCO.2022.40.6_suppl.362
3. Fotivda. Prescribing information. AVEO Pharmaceuticals Inc; 2021. Accessed January 18, 2023. https://bit.ly/405Wyr1
4. Cabometyx. Prescribing information. Exelixis Inc; 2021. Accessed January 18, 2023. https://bit.ly/3ZV4Bqm
5. Inlyta. Prescribing information. Pfizer Inc; 2022. Accessed January 18, 2023. https://bit.ly/3kwTeVl
6. Lenvima. Prescribing information. Eisai Inc; 2022. Accessed January 18, 2023. https://bit.ly/3Jgr9Mr
7. Afinitor. Prescribing information. Novartis Pharmaceuticals Corporation; 2022. Accessed January 18, 2023. https://bit.ly/3JfUI0x
8. Nexavar. Prescribing information. Bayer HealthCare Pharmaceuticals Inc; 2020. Accessed January 18, 2023. https://bit.ly/3H82lDB
9. FDA approves tivozanib for relapsed or refractory advanced renal cell carcinoma. FDA. Updated March 10, 2021. Accessed January 18, 2023. https://bit.ly/3kJqd9d










Enhancing Precision in Immunotherapy: CD8 PET-Avidity in RCC
March 1st 2024In this episode of Emerging Experts, Peter Zang, MD, highlights research on baseline CD8 lymph node avidity with 89-Zr-crefmirlimab for the treatment of patients with metastatic renal cell carcinoma and response to immunotherapy.
Listen

Beyond the First-Line: Economides on Advancing Therapies in RCC
February 1st 2024In our 4th episode of Emerging Experts, Minas P. Economides, MD, unveils the challenges and opportunities for renal cell carcinoma treatment, focusing on the lack of therapies available in the second-line setting.
Listen



