Early Study Shows Promise for Novel BET Inhibitor in Progressive Lymphomas
A novel bromodomain and extra terminal protein inhibitor demonstrated promising early activity and a manageable safety profile in the treatment of patients with relapsed or refractory lymphoma in the results of a first-in-human phase I trial.


A novel bromodomain and extra terminal protein (BET) inhibitor demonstrated promising early activity and a manageable safety profile in the treatment of patients with relapsed or refractory lymphoma in the results of a first-in-human phase I trial.
“CPI-0610 is a well-tolerated, oral BET inhibitor. The major [adverse] effect is thrombocytopeniathat is a class effect and it is reversible and noncumulative,” said Adrian Senderowicz, MD, of Constellation Pharmaceuticals, who presented the findings during the 2018 International Congress on Targeted Anticancer Therapies.
CPI-0610 is an oral potent and selective BET bromodomain inhibitor. Senderowicz noted that “the regulation of BET proteins can modulate critical signaling pathways for oncology: MYC, BCL2, NF-kβ target genes, and TGF-β target genes.”
The phase I 0610-01 trial was 1 of 3 phase I studies examining the potential of the BET inhibitor. The dose-escalation study in patients with progressive lymphoma had a 3+3 design and evaluated doses from 6 mg to 300 mg in capsule form and at 125 mg or 225 mg in tablet form. Across all doses, the schedule was 14 days on and 7 days off.
Patients in the study had relapsed or refractory non-Hodgkin or Hodgkin lymphoma who were not eligible for or who had relapsed after high-dose chemotherapy or transplant. The primary endpoint of the study was the maximum-tolerated dose for CPI-0610, and secondary endpoints included safety, tolerability, pharmacokinetics, preliminary antitumor effects, and pharmacodynamics.
Sixty-four patients were included in the trial across the 11 investigated doses. Of these, 75% were male and the median age was 63 years. Most patients were heavily pretreated with a median of 4 prior therapies (range, 1-12).
The majority of the patients (56.3%) had diffuse large B-cell lymphoma, 12.5% had follicular lymphoma, 7.8% had Hodgkin lymphoma, 4.7% had mantle cell lymphoma, and 18.8% had a different lymphoma diagnosis.
The most common (≥5%) treatment-related adverse events across all doses and across both forms of treatment was thrombocytopenia (42.2%), nausea (17.2%), and fatigue (17.2%). No cases of thrombocytopenia were observed in patients who received doses of 50 mg or lower.
The study included a broad view of dose-limiting toxicities (DLTs) (TABLE). Hematologic DLTs were observed in 4 patients, including 1 patient who developed grade 3 neutropenic fever at the 80-mg capsule dose. Grade 4 thrombocytopenia was experienced by 3 patients, including 1 on the 230-mg capsule dose, another on the 300-mg capsule, and a third who was receiving the 225-mg tablet. Two of the 3 patients recovered within 2 weeks.
Nonhematologic DLTs included 1 grade 3 rash at 48 mg, and 2 cases of grade 3 diarrhea, 1 at 170 mg and another at 230 mg. Each of the nonhematologic DLTs were resolved.


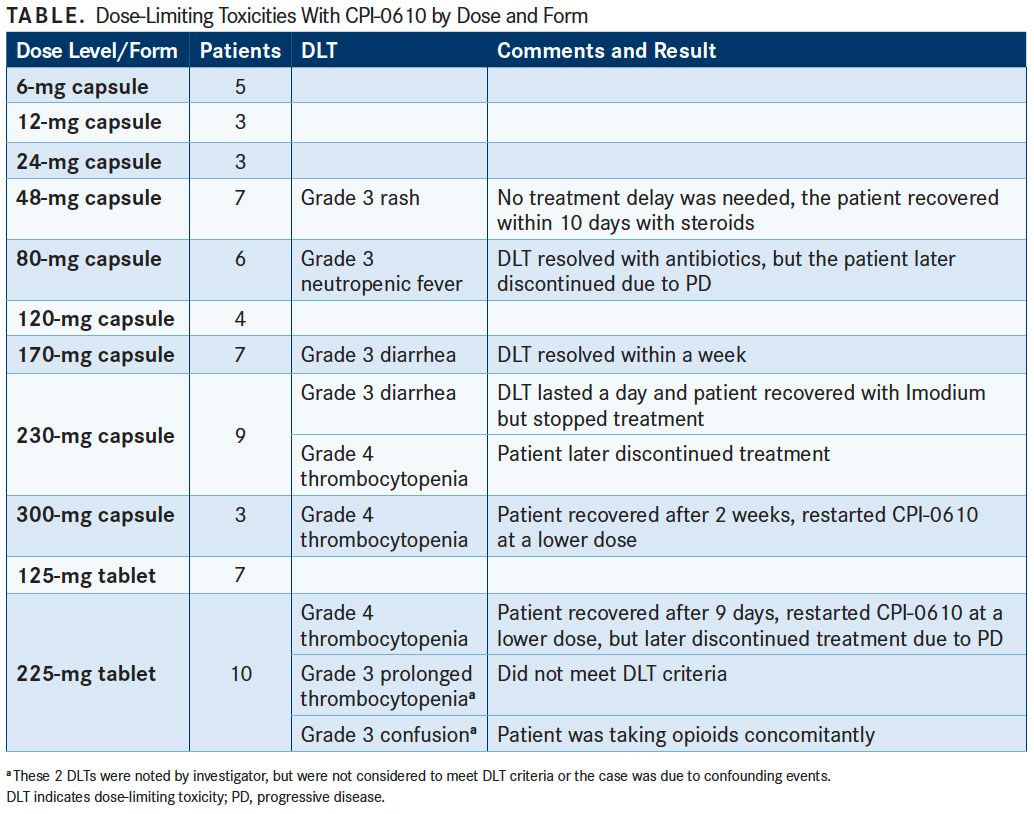
The maximum-tolerated dose was deemed to be 225 mg in tablet form, which was also based on DLTs found in the other phase I studies.
Among 38 patients evaluable for efficacy analysis, 5 objective responses (13.2%) were observed, including 2 complete responses (CRs) and 3 partial responses (PRs). Three of 5 patients with activated B-cell diffuse large B-cell lymphoma experienced a response, consisting of 1 CR and 2 PRs. The second CR was achieved in a patient with T-cell histiocyte rich B-cell lymphoma and 1 patient with follicular lymphoma had a PR. Senderowicz added that 17 other patients experienced some degree of tumor shrinkage.
In the pharmacokinetics analysis of CPI-0610 across the doses studied, the investigators noted dose proportional increases in exposure across the 6-mg to 170-mg capsule doses with similar exposure observed across the 170-mg to 300-mg doses. However, the tablet form was recommended for further investigation. “The bioavailability of the tablets is approximately 40% higher than the capsules,” he said.
IL8 and CCR1 mRNA levels were both evaluated in peripheral blood mononuclear cells for treatment effects. CPI-0610 rapidly suppressed expression of both proinflammatory cytokines. “There is a dose-dependent and concentration-dependent inhibition of IL8 and CCR1, and both are NF-kB dependent genes,” Senderowicz said. Maximal effects were observed 2 hours after treatment.
Based on preclinical data and significant clinical effects on proinflammatory cytokines, a phase II trial has also begun looking at CPI-0610 either with or without ruxolitinib (Jakafi) in myelofibrosis in the second-line setting (NCT02158858).
Reference:
Blum KA, Abramson J, Maris M, et al. A phase I study of CPI-0610, a bromodomain and extra terminal protein (BET) inhibitor in patients with relapsed or refractory lymphoma. Presented at: TAT 2018 Targeted Anticancer Therapies; March 5-7, 2018; Paris, France. Abstract 410.












Survivorship Care Promotes Evidence-Based Approaches for Quality of Life and Beyond
March 21st 2025Frank J. Penedo, PhD, explains the challenges of survivorship care for patients with cancer and how he implements programs to support patients’ emotional, physical, and practical needs.
Read More



Examining the Non-Hodgkin Lymphoma Treatment Paradigm
July 15th 2022In season 3, episode 6 of Targeted Talks, Yazan Samhouri, MD, discusses the exciting new agents for the treatment of non-Hodgkin lymphoma, the clinical trials that support their use, and hopes for the future of treatment.
Listen



