Roundtable Discussion: Riess Looks at the Options in Treating High PD-L1 NSCLC
During a Targeted Oncology case-based roundtable event, Jonathan Wesley Riess, MD, MS, discussed the case of a 72-year-old patient with non–small cell lung cancer with high PD-L1 expression.





Medical Director, Thoracic Oncology
UC Davis Comprehensive Cancer Center
Sacramento, CA")
Jonathan Wesley Riess, MD, MS (Moderator)
Medical Director, Thoracic Oncology
UC Davis Comprehensive Cancer Center
Sacramento, CA


RIESS: In the context of this patient being highly positive for PD-L1, [with non–small cell lung cancer (NSCLC)], your options are a PD-1 or PD-L1 antibody alone or with chemotherapy, which many people voted for. Then there’s also the IMpower150 study [NCT02366143] regimen of carboplatin, paclitaxel, bevacizumab [Avastin], and atezolizumab [Tecentriq].
The KRAS G12C inhibitor is an exciting new option to finally have that targets KRAS-mutant NSCLC. It is approved as a second-line treatment. It does have a response rate of [approximately] 40%, and the progression-free survival [PFS] is [approximately] 7 months.
KRIJANOVSKI: I would choose single-agent PD-1 or PD-L1 therapy because [my patients] have had a nice response to it. After 2 months of therapy, if I don’t see a significant response in my patient, I would add chemotherapy at that point, but if they respond nicely I don’t have to change and they can continue for 2 years.
RIESS: [For patients with] high PD-L1 expression, single-agent PD-1 or PD-L1 therapy has FDA approval as it spares [patients] the adverse effects [AEs] of chemotherapy. Potentially you can add on chemotherapy if they have an inadequate response or clinical benefit. That makes a lot of sense.
HARRIS: I didn’t pick single-agent PD-L1 [therapy but chose it in] combination [with chemotherapy] because of my previous experience with a patient in this situation where they had very high PD-L1. I gave a [patient] pembrolizumab [Keytruda] alone and she had a nice response for 3 months but a repeat CT scan showed that it was a mixed response and some of her metastatic lesions were growing. [At the time] I didn’t have a lot of data about what to do. Do I continue the pembrolizumab and add chemotherapy or give chemotherapy alone? I think I ended up [adding chemotherapy] to pembrolizumab and she got a complete clinical remission.
As far as I know, she’s still alive and doing well. I had those mixed responses and I didn’t know what to do. Now in these kinds of patients, especially the ones who are symptomatic at the outset, I’ll give combined PD-L1 and chemotherapy.
RIESS: I think that’s a rational approach too. I think both single agent and the combination are FDA approved in the setting with high PD-L1. I think you did what most would do, which would be to layer on the chemotherapy to the immunotherapy because there was evidence she was failing because of the mixed response. Cross-trial comparisons all have their pitfalls, but chemotherapy plus immunotherapy and immunotherapy alone in this setting have not been compared head-to-head. We’re doing that in a subset of the INSIGNA trial [NCT03793179]; that’s a National Cancer Institute [NCI]–sponsored trial, and we have it open at UC [University of California] Davis. I agree that in patients who need a response, chemotherapy plus immunotherapy has a potentially higher response, although they haven’t been directly compared.
CHO: Would you consider adding chemotherapy too, knowing that she’s KRAS positive? Are there any such data?
RIESS: If a patient has an exceptionally high PD-L1 score, [such as] this patient with 95%, I typically do single-agent PD-1 or PD-L1 therapy if I feel they don’t need a response because it spares them the chemotherapy AEs. I could save it for later if response rates are [higher than] 40%, there are durable responses, and PFS. If I feel [as though] they’re symptomatic and they need a response as was mentioned, I give chemotherapy plus immunotherapy.
I distinguish [among] KRAS G12C and BRAF mutations and EGFR, ALK, ROS1, and so forth. EGFR and ALK were excluded from a lot of these trials, and you could extrapolate ROS1 too. A lot of never- and light-smoking patients with lung cancers with these oncogene drivers would not likely benefit from single-agent immunotherapy. KRAS G12C seems to be a bit different because it’s a smoking-associated mutation, so these patients can do very well with immunotherapy.
The KRAS G12C would not dissuade me from single-agent immunotherapy. If I had a patient with an ERBB4 mutation, which is similar to EGFR (ERBB1), that we don’t have a targeted agent for and they are a never-smoker, I’m going to give him chemotherapy plus immunotherapy and not immunotherapy alone because I’m not confident that type of patient is going to have a response reflective of the overall population in some of these trials. That’s how I practice.
CHEN: If this patient had a PD-L1 of 50% vs 95%, would you treat them differently? Would you be more likely to give chemotherapy plus immunotherapy vs immunotherapy alone?
RIESS: I take it into consideration and if I don’t think they are going to get in trouble, then I would probably still do single-agent immunotherapy. If you get a great response and avoid the patient having the potential AEs of chemotherapy, I think there’s an advantage there. If I think the [patient is] symptomatic and they could get into trouble soon, I would be more likely to give chemotherapy plus immunotherapy. It factors into the whole holistic decision-making.
ONWERE: Have you seen any increased risk of ILD [interstitial lung disease] if you give immunotherapy first, followed by the KRAS G12C inhibitor treatment?
RIESS: I don’t think that’s been reported but it is a great question, and I don’t know the answer to it. Certainly, it is true that osimertinib [Tagrisso] after PD-1 [therapy has a] high risk of pneumonitis. The trials were stopped for pneumonitis, but also the drugs bound to the receptor for 3 months. I worry about liver function test abnormalities and so forth, but I don’t think we know yet for sotorasib [Lumakras], I’d have to look at the data. I don’t believe it’s nearly as dramatic. I would still have confidence giving it because keep in mind it is approved as a second-line therapy. So I would not be dissuaded from using it, but I would be leery with osimertinib, alectinib [Alecensa], and so forth.



EY: I voted for chemotherapy plus immunotherapy because the patient had a high disease burden and a great performance status. This is my devil’s advocate comment.
As you know, the KEYNOTE trials are all funded by Merck and we all know that adding immunotherapy to chemotherapy is good and we all know that immunotherapy is better than chemotherapy, but no one’s bothered to pay for the trial to show if we need immunotherapy plus chemotherapy. The Bristol Myers Squibb trials of the paclitaxel plus carboplatin regimen back in the day were well funded, but nobody cares anymore about chemotherapy. So a somewhat naughty comment, if you will, but the money’s in the new drugs, so studies to determine the benefit of chemotherapy when no one can make any money on it are lacking.
RIESS: You bring up some good points. Between chemotherapy plus immunotherapy and immunotherapy alone, there’s no right or wrong.
EY: Yes, and [there are] no data.
RIESS: I would say in terms of the trials, NCI is paying for the INSIGNA trial and we have it open at UC Davis. It randomizes patients to chemotherapy plus immunotherapy vs immunotherapy alone. It’s for patients with PD-L1 of 1% or greater, but I think the most interesting question is in the subset of 50% or greater and then crossing over to different maintenance strategies for the single-agent immunotherapy arm upon progression.
EY: It will happen eventually; it’s just that the Merck-sponsored trials got to market a whole lot faster for obvious reasons.
RIESS: Those are all good points, but there is a trial that hopefully will have enough of those patients at least as a subset to try to answer that question.



EY: I will just say that’s what I’ve used the most and I’m used to it. I don’t know if one’s any better than another, but I’m very interested in cemiplimab [Libtayo]. I haven’t used it yet because it just got approved.
MITIN: I’m a radiation oncologist. The patient did not receive radiation therapy to the brain, and there is only 1 prospective Merck study that was done at Yale [University], where they used pembrolizumab alone without treating brain metastases and they did not lose any patients. They had good response rates and disease control, so I would be certainly in favor of pembrolizumab in this situation.
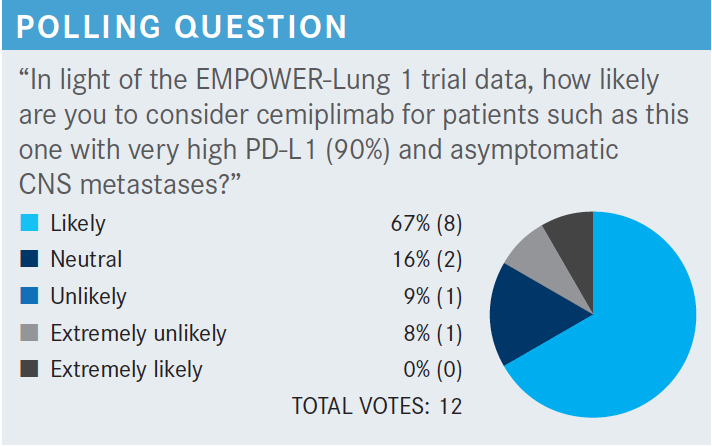
RIESS: There is an intracranial response [with pembrolizumab in] the KEYNOTE-024 study [NCT02142738] and cemiplimab in the EMPOWER-Lung 1 study [NCT03088540]. They allowed [patients with] treated brain metastases. There is a response rate associated with immunotherapy. I would say overall from both retrospective and prospective trials, it is [approximately] 20%. It’s not like osimertinib in EGFR lung cancer or alectinib in ALK lung cancer where you’re looking at high intracranial response rates.1,2
GOLDBERG: I think familiarity [with the drug] is important when things are equal.
ONWERE: Are the other agents used as single agents in high PD-L1 NSCLC?
RIESS: Yes. We’ll go through the cemiplimab data in more detail. Pembrolizumab, cemiplimab, and atezolizumab all have approval as single agents in PD-L1–high NSCLC. Cemiplimab and pembrolizumab used the 22C3 assay, which is the most common. The atezolizumab has the TC3, TCIC Ventana assay, which is a bit different, although for all intents and purposes in high PD-L1 there’s a decent correlation.
CHEN: It seems for anti–PD-1 and anti–PD-L1, the efficacy, safety, and tolerability are similar. I like that in pembrolizumab—you have the option of 6-week dosing, so logistically for some patients it’s a lot easier.
RIESS: The 6-week dosing makes a difference for some patients, especially those coming from a distance. I would note that cemiplimab is FDA approved for advanced cutaneous squamous cell carcinoma too.
SUPERFIN: I have a question. Most recently we got into the Signatera [tests]….I have a patient with bladder cancer [on treatment] for 2 years and I’m going to test it on them and see if we should stop or continue therapy. Have you ever used any markers [such as] minimal residual disease [MRD] markers?
RIESS: That’s a great point. I have not, but I think monitoring MRD and whether to stop or not and whether that improves outcome [will be] an area for further study.
The trials used ICIs for 2 years and then stopped. Patients could be rechallenged if they progressed again.
In the publication from the KEYNOTE-024 study, for example, some patients can still re-respond.1 I have patients who feel strongly though, so it’s always an interesting discussion. I have sometimes [given radiation to] those with residual disease.
BEHL: I do stop and, in fact, when I explain to the patients that they are doing well but AEs can happen at any time and they can be devastating, most come around and agree to stop. I then tell them that we will still be monitoring and if the cancer comes back, we can restart therapy.
EY: I haven’t had a lot of patients go to 2 years because they get tired. I think a lot of them stop sooner because of increasing fatigue and obviously there are occasional ones who stop for specific organ toxicities. If somebody was doing great and had no AEs at 2 years, I’d probably continue, at least offer it or allow it. I haven’t had too many [patients] who do not want to stop after 2 years.
RIESS: It’s a minority of patients in this position. It’s always a fortunate discussion in some ways, but it could be challenging. I discuss stopping as well at 2 years because that’s what the trials do, but I don’t think we know for sure.
ONWERE: It’s an easy sell if they’ve had a CR [complete response] for 2 years.
RIESS: That’s true.
CHO: In the pembrolizumab study, did it show any CNS activity?
RIESS: Treated brain metastases were allowed in both the KEYNOTE-024 and the EMPOWER-Lung 1 study with pembrolizumab and cemiplimab, respectively. I would say that some patients may have had Gamma Knife [surgery], for example, for the brain lesion before. It’s always challenging if you’re pressed to treat [a patient] with the timeline for Gamma Knife. I feel comfortable doing overlapping immunotherapy and Gamma Knife surgery when you need to treat. I certainly would have sent this patient for a discussion with radiation oncology regarding that.
If you look at untreated brain metastases, there are smaller retrospective and prospective studies showing [intracranial] response rates in general anywhere from 13% to 30%, but of course that’s not necessarily in high PD-L1 where you’d anticipate they may have a higher intracranial response rate.


ONWERE: I think that [alternate single-agent ICIs, pembrolizumab and atezolizumab,] are all great options. I’ve just used pembrolizumab for a very long time.
RIESS: Would anybody face any barriers to the use of a new single-agent ICI, institutional or otherwise?
BEHL: Yes, if it’s not on the institutional pathways then you must have a good justification of why you want that.
RIESS: Is there any scenario in which one would consider an alternative single-agent ICI to pembrolizumab or atezolizumab?
HARRIS: I guess if the cost is significantly lower, then that would get the attention of our pharmacy financial people. I think then they would say we would like to offer this as a favorable alternative if the results are comparable. But most of the time the new drugs come out and they’re just as expensive or more expensive than what we’ve been using, so they don’t get an inside track at all.
BEHL: If it’s oligo-progression and if we can get by with radiation, then I would offer radiation and continue the ICI depending on how long they’ve responded and how well.
RIESS: I’ve done that, too, especially for intracranial progression but also systemic progression. For oligo-progression I [use radiation] and continue. I think you can often buy extra time by doing so. This patient had more diffuse progression, so what would one do in the setting of diffuse progression?
BEHL: Then it’s time to consider chemotherapy.
RIESS: Who would do chemotherapy and drop the immunotherapy vs layer on the chemotherapy in this situation?
BEHL: I think it depends on how much mileage you’ve got with the immunotherapy.
ONWERE: I always layer [with chemotherapy].
REISS: I practice the same way. There’s no right answer, but if somebody had high PD-L1 with some 6-month PFS benefit and you hoped for more, I would layer on [chemotherapy] as well if they tolerated it. For patients who progress dramatically right away, I usually take it off. For example, if they progress on durvalumab [Imfinzi], I often will just do the chemotherapy alone.
HARRIS: For the single site of progression, would you ever consider a lateral adrenalectomy rather than radiation?
RIESS: I would. I think it depends on the patient, but…preimmunotherapy there were data for that, particularly for a single adrenal metastasis. It depends on the situation, but if it was just an adrenal metastasis, that’s something I would consider.
MITIN: As a radiation oncologist, I typically think that putting patients through surgery would require them to be off systemic therapy for a while, so radiation therapy offers that advantage of continuing systemic therapy and getting the ablative treatment.
HARRIS: Are there any data comparing surgical approach vs radiation?
MITIN: No, there are no data comparing them. Patients who go for surgery typically have potentially better survival data than patients who go for radiation therapy. There is a patient selection bias but certainly…radiation therapy on adrenal metastases achieves a good local control and it’s usually well tolerated by patients.
CHEN: If the patient doesn’t want chemotherapy to be added on to the immunotherapy, are there data to support adding ipilimumab [Yervoy] to the pembrolizumab?
RIESS: There aren’t, but there are 2 studies I would highlight. One is the nivolumab [Opdivo] plus ipilimumab Lung-MAP substudy [NCT02785952], which was terminated early because of the changing landscape where it looked like there wasn’t much of a response rate. I would note that Merck did a trial of pembrolizumab plus ipilimumab [in patients with high] PD-L1, and it was not better than pembrolizumab alone. I do not add ipilimumab in this situation. If the patient didn’t want chemotherapy, like for a patient with KRAS G12C mutation, you’ve got sotorasib, which will give you [approximately] a 40% response rate and a PFS of [approximately] 7 months on average. I think that’s another nuance.
Would you do sotorasib or would you do chemotherapy layered on to immunotherapy? I think once again there’s not a right answer for that. I think I would have a discussion with the patient about it. Certainly, immunotherapy and sotorasib together is not an approved regimen and we’re still learning more about that. There’s some sense that there may be some increased toxicity, but we don’t know. If I thought they were deriving some benefit from immunotherapy, I’d probably layer the chemotherapy on first.
SUPERFIN: Have you ever tried sotorasib on other KRAS mutations?
RIESS: It didn’t work. It’s a direct inhibitor of KRAS G12C that traps the G12C and it’s an active noncycling form. It doesn’t bind to any of the other KRAS amino acid substitutions. There are some pan-RAF inhibitors, and we have a bunch of trials at UC Davis looking at some interesting drugs for the non-G12C KRAS mutations. But sotorasib and the direct KRAS G12C inhibitors won’t work against other KRAS mutations.
REFERENCES
1. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non–small-cell lung cancer. N Engl J Med. 2016;375(19):1823-1833. doi:10.1056/NEJMoa1606774
2. Sezer A, Kilickap S, Gümüş M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021;397(10274):592-604. doi:10.1016/S0140-6736(21)00228-2






















