Durvalumab Combo, With or Without Tremelimumab, Improves PFS in NSCLC
Data from the phase 3 POSEIDON trial were presented during the International Association for the Study of Lung Cancer 2021 World Conference on Lung Cancer.


Melissa L. Johnson, MD

Durvalumab (Imfinzi) and chemotherapy, with or without tremelimumab, demonstrated statistically significant improvement in progression-free survival (PFS) compared with chemotherapy alone in patients with metastatic non–small cell lung cancer (NSCLC).
Data from the phase 3 POSEIDON trial (NCT03164616) were presented during the International Association for the Study of Lung Cancer 2021 World Conference on Lung Cancer.1
The median PFS with durvalumab/chemotherapy was 5.5 months (95% CI, 4.7-6.5) compared with 4.8 months (95% CI, 4.6-5.8) for chemotherapy alone, leading to a 26% reduction in the risk of disease progression or death (HR, 0.74; 95% CI, 0.62-0.89; P = .00093) (TABLE).
However, the median overall survival (OS) was 13.3 months (95% CI, 11.4-14.7) with durvalumab/ chemotherapy and 11.7 months (95% CI, 10.5-13.1) with chemotherapy alone—a difference that was not found to be statistically significant (HR, 0.86; 95% CI, 0.72-1.02; P = .07581).
Conversely, when tremelimumab was added to the durvalumab/chemotherapy regimen, both the PFS and OS benefits of chemotherapy were statistically significant, explained lead study author Melissa L. Johnson, MD, who presented the data virtually in a press briefing during the meeting.
Specifically, the median PFS was 6.2 months (95% CI, 5.0-6.5) vs 4.8 months (95% CI, 4.6-5.8) with chemotherapy alone (HR, 0.72; 95% CI, 0.60-0.86; P = .00031). The median OS was 14.0 months (95% CI, 11.7-16.1) and 11.7 months (95% CI, 10.5-13.1) in the 3-drug and chemotherapy-alone arms, respectively (HR, 0.77; 95% CI, 0.65- 0.92; P = .00304).
“We noticed an improved separation of the curves with the addition of tremelimumab, and improvement in both the 12-month PFS as well as the 24-month OS landmark analysis over what was seen with durvalumab plus chemotherapy,” Johnson, program director of lung cancer research at Sarah Cannon Research Institute, said. “Durvalumab plus tremelimumab plus chemotherapy represents a potential new frontline treatment option for patients with metastatic NSCLC.”
Although PD-1/PD-L1 inhibitors have transformed the treatment paradigm of advanced NSCLC, both as single agents and in combination with chemotherapy, an unmet need remains for this population. The addition of CTLA-4 inhibition to PD-L1 antibodies and chemotherapy, however, could confer further clinical and long-term survival benefit in select patient subgroups.
In the international, open-label, multicenter POSEIDON trial, investigators explored durvalumab, with or without tremelimumab, in combination with investigator’s choice of chemotherapy in the frontline treatment of patients with squamous or nonsquamous metastatic NSCLC (n = 1013). Patients were randomized 1:1:1 to receive durvalumab 1500 mg plus chemotherapy every 3 weeks for 4 cycles, followed by maintenance durvalumab 1500 mg every 4 weeks plus pemetrexed until disease progression (n = 330); durvalumab 1500 mg plus tremelimumab 75 mg and chemotherapy every 3 weeks for 4 cycles, followed by maintenance durvalumab 1500 mg every 4 weeks plus tremelimumab 75 mg at week 16 only, and pemetrexed until disease progression (n = 335); or platinum-based chemotherapy every 3 weeks for up to 6 cycles, followed by maintenance pemetrexed until disease progression (n = 332).
Primary end points were PFS by blinded independent central review (BICR) and OS for durvalumab/chemotherapy vs chemotherapy alone. Secondary end points were PFS by BICR and OS, as well as OS in patients with blood tumor mutational burden (≥20 mutations per megabase) for durvalumab/tremelimumab plus chemotherapy vs chemotherapy alone.
Additional outcome measures included objective response rate (ORR), duration of response (DOR), and best objective response by BICR, as well as 1-year PFS rate, health-related quality of life, safety, and tolerability.
Additional findings presented at the meeting showed that in the durvalumab/chemotherapy and chemotherapy-alone arms, the 1-year PFS rates were 24.4% and 13.1%, respectively. The 2-year OS rates were 29.6% and 22.1%, respectively. With the addition of tremelimumab to durvalumab/chemotherapy, the 1-year PFS rate was 26.6% and the 2-year OS rate was 32.9%.
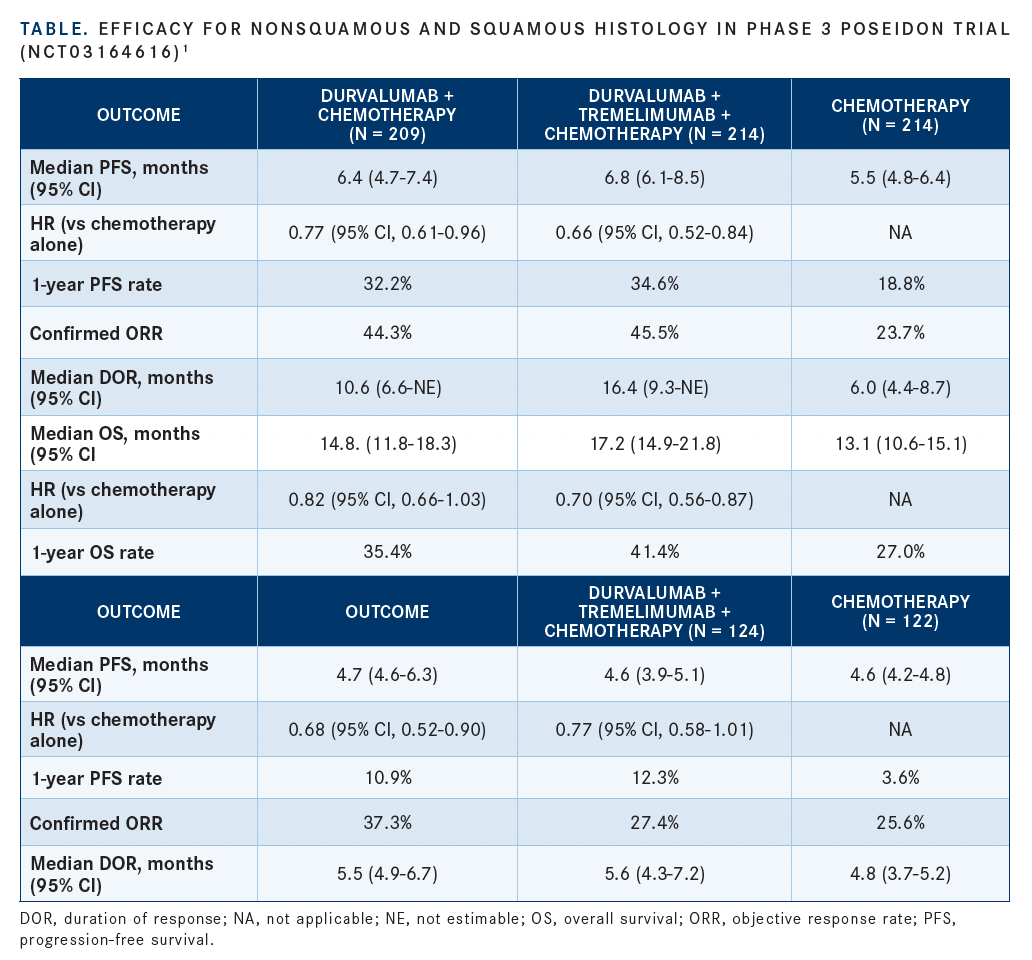
Johnson said that the addition of tremelimumab to durvalumab/chemotherapy appeared to have the highest benefit in patients with nonsquamous histology.
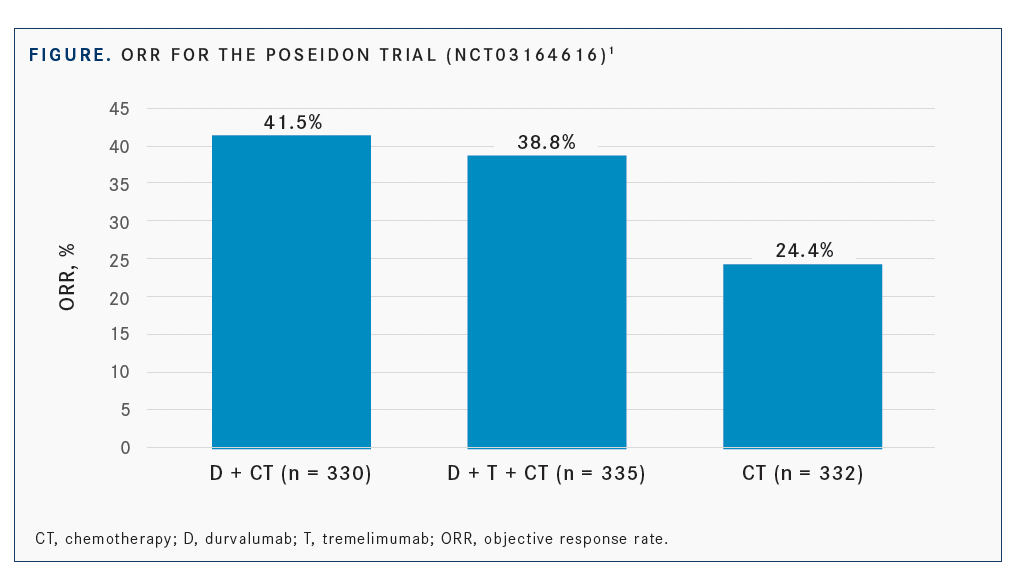
The confirmed ORRs were 41.5% with durvalumab/chemotherapy, 38.8% with durvalumab/tremelimumab plus chemotherapy, and 24.4% with chemotherapy alone (FIGURE). The odds ratio was 2.26 (95% CI, 1.61-3.19) between durvalumab/chemotherapy and chemotherapy alone and 2.00 (95% CI, 1.43- 2.81) between durvalumab/tremelimumab plus chemotherapy and chemotherapy alone.


Additionally, the DOR was 7.0 months (95% CI, 5.7-9.9), 9.5 months (95% CI, 7.2-not estimable), and 5.1 months (95% CI, 4.4-6.0) for durvalumab/chemotherapy, durvalumab/chemotherapy plus tremelimumab, and chemotherapy alone, respectively. At 12 months, 38.9%, 49.7%, and 21.4% of these patients maintained a response, respectively.


The trial investigators observed no unexpected safety signals, and most adverse events (AEs) were driven by chemotherapy.
All-grade, all-cause AEs occurred in 96.1%, 97.3%, and 96.1% of patients who received durvalumab/chemotherapy, durvalumab/chemotherapy plus tremelimumab, and chemotherapy alone, respectively; the rates of grade 3/4 AEs in these groups were 54.8%, 53.3%, and 51.7%, respectively. Serious AEs occurred in 40.1% of patients receiving durvalumab/chemotherapy, 44.2% receiving durvalumab/chemotherapy plus tremelimumab, and 35.1% receiving chemotherapy alone.
Treatment discontinuation (20.4%, 22.1%, and 15.3%, respectively) and death rates (10.2%, 12.4%, and 9.0%, respectively) due to AEs were similar across all 3 arms, Johnson noted.
All-grade treatment-related AEs (TRAEs) occurred in 88.6% of patients on durvalumab/chemotherapy, 92.7% who received the addition of tremelimumab, and 89.5% of patients receiving chemotherapy. Grade 3/4 TRAEs occurred in 44.6%, 51.8%, and 44.4% of patients, respectively.
Serious TRAEs were experienced by 19.5% of patients who received durvalumab/chemotherapy, in 27.6% receiving durvalumab/ tremelimumab plus chemotherapy, and in 17.7% receiving chemotherapy alone. TRAEs that led to drug discontinuation occurred in 14.1%, 15.5%, and 9.9% of patients, respectively; TRAEs that led to death were reported in 2.1%, 3.3%, and 2.4% of patients, respectively.
REFERENCE:
1. Johnson ML, Cho BC, Luft A, et al. Durvalumab ± tremelimumab + chemotherapy as first-line treatment for mNSCLC: results from the phase 3 POSEIDON study. Presented at: International Association for the Study of Lung Cancer 2021 World Conference on Lung Cancer; September 8-14, 2021; Virtual. Abstract PL02.01.

















