Study Shows AKT1 E17K a Targetable Mutation Through AKT Inhibition Across Various Cancer Types
Amultihistology basket study proved the targetability of the <em>AKT1 E17K</em> mutation in human cancers by treating patients with various types of cancer harboring an <em>AKT1 E17K </em>mutation with AZD5363, an oral pan-AKT inhibitor, according to findings published in the <em>Journal of Clinical Oncology</em>.
David Hyman, MD
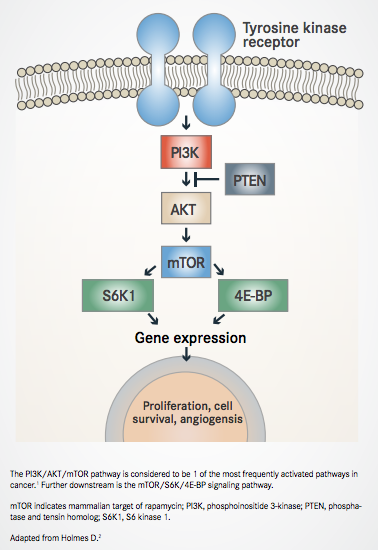
Amultihistology basket study proved the targetability of theAKT1 E17Kmutation in human cancers by treating patients with various types of cancer harboring anAKT1 E17Kmutation with AZD5363, an oral pan-AKT inhibitor, according to findings published in theJournal of Clinical Oncology.1The PI3K/AKT pathway is one of the most frequently activated pathways across cancers and can be triggered by one of several mutations.
Although theAKT1 E17Kmutation can be found in many cancer types, they nonetheless occur at a relatively low prevalence in individual tumor lineages despite being the most commonAKT1mutation. The oncogenic nature of these gain-of-function mutations means they can be targeted with an AKT inhibitor in the hopes of improving patient outcomes.
The safety and efficacy of the AKT inhibitor had previously been investigated in patients withPIK3CA-mutant estrogen receptor (ER)-positive breast cancer, HER2-positive breast cancer, or gynecologic cancers. Three of 51 patients experienced a partial response, and the optimal dose and schedule for AZD5363 was set.
In the basket study of patients withAKT1mutations, 58 heavily pretreated patients were enrolled to receive 480 mg twice daily of AZD5363 on a 21-day cycle for 4 days followed by 3 days off, repeated weekly.
Of the enrolled patients, 52 showed expression of an E17K mutation, 2 patients had anE79Kmutation, and 1 each had anF35L, T34N,orV201Amutation; one patient had an undetectable mutation. Patients were a median 59 years (range, 31-77) and had received a median of 5 treatment regimens (range, 1-14). A majority of the patients (91.4%) were female and had a WHO performance status of 1 (53.4%); the remainder had a performance status of 0.
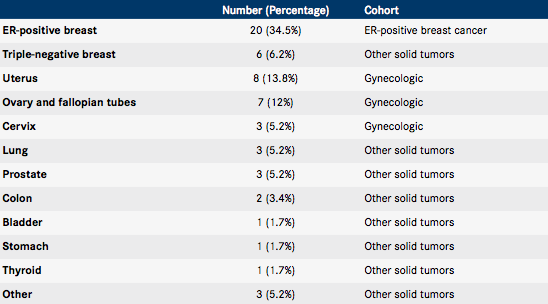
Following enrollment, patients were divided into 3 cohorts based on the location of their primary tumor: ER-positive breast cancer (n = 20), gynecologic cancers (n = 18), and other solid tumors (n = 20) (Table).
Table. Primary tumor location of enrolled patients1


Once treatment commenced, patient disease was assessed and analyzed at baseline, every 6 weeks for 6 months, then every 12 weeks until any occurrence of a significant change in progression or withdrawal. The primary endpoint of this study was safety; response according to RECIST v1.1 criteria and progression-free survival (PFS) were key secondary endpoints.
Partial responses were confirmed in AKT1 E17K-mutant patients, including in 4 patients with ER-positive breast cancer, 2 with endometrial cancer, and 1 patient each with cervical cancer, triple-negative breast cancer, and lung adenocarcinoma. One patient with ovarian cancer with a Q17K mutation experienced stable disease and tumor regression lasting 14 months.
In treated patients with E17K mutations, the median
PFS was 5.5 months (95% CI, 2.9-6.9) for patients with ER-positive breast cancer, 6.6 months (95% CI, 1.5-8.3) for gynecologic cancers, and 4.2 months (95% CI, 2.1-12.8) for other solid tumor types. Researchers concluded that there was no apparent correlation between tumor type and response.
Grade ≥3 adverse events (AEs) were observed in 70.7% of patients, and 51.7% were deemed to have a casually related AE, as assessed by the investigator. Hyperglycemia (24.1%), diarrhea (17.2%), and maculopapular rash (15.5%) were the common grade ≥3 AEs reported. A dose reduction was necessitated in 34% of patients, with the above AEs being the leading causes. Serious AEs were experienced by 15.5% of patients, and the authors, led by David M. Hyman, MD, chief of the Early Drug Development Service at Memorial Sloan Kettering Cancer Center, noted that the toxicity profile was consistent with that of previous studies with AZD5363.
Prior to treatment, researchers collected and sequenced tumor samples and tumor-derived cell-free DNA (cfDNA) for retrospective and comparative analysis purposes and to see whether response could be predicted through examination of biomarkers. Interestingly, in 1 evaluable sample in which theAKT1 E17Kmutation could not be confirmed in either cfDNA or archival tumor, the patient experienced rapid disease progression.
During cycle 1, a ≥50% decrease in theAKT1 E17Kmutant allele in cfDNA was observed in 22 of 23 patients (95.5%) that showed no correlation with response. Observations of an ongoing decrease in mutant alleles going into cycle 2 showed an association with an increase in PFS (median PFS, 5.6 vs 2.6 months in those who did not demonstrate a decline; HR, 0.18;P= .004). Five patients experienced a clearance ofAKT1 E17Kmutant alleles in cfDNA lasting more than 21 days that correlated with objective responses lasting ≥18 weeks (P= .025).
Through whole-exome or targeted sequencing in a smaller population of patients (n = 37), researchers tested to see if there was a correlation between the genomic configuration of the mutation and response to AZD5363. An allelic imbalance ofAKT1 E17Kwas observed in 57% of the tested patients (n = 21). Further testing revealed that 10 of these patients exhibited a copy-neutral loss of heterozygosity (CN-LOH), whereby 1 patient had acquired 2 copies of a mutant AKT1 E17K allele with no remaining wild-type allele. The authors noted that those patients experienced a longer PFS than those who did not exhibit CN-LOH (median PFS, 8.2 vs 4.1 months, respectively; HR, 0.41;P= .04), and they found this association to be clinically and statistically significant. Furthermore, they concluded that this E17K allelic imbalance was more commonly found in patients with breast or gynecologic cancers (90% vs 10% of other tumor types).
Clonality, or degree of tumor cell presence, of theAKT1 E17Kmutation may have some type of correlation with respones to AZD5363. Although 92% of patients (34 of 37) hadAKT1 E17Kmutations present in all tumor cells, 2 of the remaining 3 patients with subclonal mutations exhibited a rapid increase in disease progression, and the third patient, who had ovarian granulosa cell cancer, experienced a mixed response. Hyman and his colleagues suspected that the third patient’s overall tumor regression of 24% that lasted 253 days was caused by the later acquisition of theAKT1 E17Kdriver mutation, which led to a response from treatment.
Researchers also looked into the influence of commutations and concurrent activation of adjacent signaling pathways on sensitivity to inhibition. Additional mutation and activation of the PI3K/mTOR signaling pathway (Figure2) was found to correlate with longer PFS (median PFS, not reached vs 4.3 months without additional pathway mutations; HR, 0.21;P= .045). Five patients exhibited this coincident mutation in upstream or downstream effectors of signaling of the PI3K/ mTOR pathway. The potential of increased sensitivity to PI3K pathway inhibition due to concomitant pathway mutations is an area worthy of further research, the authors noted.
Figure. The PI3K/AKT/mTOR Pathway2


Other cases include an achievement of durable partial response in 2 of 5 patients with loss-of-function NF1 mutations (cervical and breast cancer), where 1 exhibited a subclonal FGFR3 S249C hotspot mutation; detection of an AZD5363- resistant subclonal KRAS A146T mutation in 1 patient with colorectal cancer; and mutations in the ligand-binding domain of ESR1 in 7 of 20 patients (35%) who experienced a shorter median PFS than those without the mutation (P= .004).
Overall, the results of this clinical study strongly suggest that AKT1 E17K mutations can be a promising target for cancer therapy. “To our knowledge, this study provides the first robust clinical evidence that AKT1 E17K is a targetable oncogene in human cancer,” the authors wrote in the study.
The authors also noted that the AZD5363 response in these mutations was greater than that seen withPIK3CAmutations, which further confirms the efficacy ofAKT1inhibition. Yet, they observed that the PFS of these treated patients was disappointingly lower than other therapeutic options targetingEGFR, ALK, ROS1,andBRAF. Thus, they suggested that AZD5363 may be most effective in a combination setting. Studies examining AKT inhibition with antiestrogen therapies are underway in patients with ER-positive,AKT1-mutant cancers.
Hyman and his co-authors feel confident that their study will illuminate further studies and advance the understanding of inhibition in a mutation-specific context. “By incorporating comprehensive tissue- and plasma-based correlative studies,” they conclude, “we elucidate the multifaceted genomic basis of response in a manner that facilitates simultaneous translational genomic discoveries and clinical hypothesis validation to inform future studies."
References:
- Hyman D, Smyth LM, Donoghue MTA, et al. AKT1 inhibition in solid tumors with AKT1 mutations. J Clin Oncol. 2017;35(20):2251- 2259. doi: 10.1200/JCO.2017.73.0143
- Holmes D. PI3K pathway inhibitors approach junction. Nat Rev Drug Discov. 2011;10(8):563-564. doi: 10.1038/nrd3527.














Survivorship Care Promotes Evidence-Based Approaches for Quality of Life and Beyond
March 21st 2025Frank J. Penedo, PhD, explains the challenges of survivorship care for patients with cancer and how he implements programs to support patients’ emotional, physical, and practical needs.
Read More




