A Decade of Breast Cancer at the Molecular Level: Pioneering Personalized Medicine
As we identify more targets...there will probably be more and newer, perhaps even better, therapeutics than we have currently, said Dennis J. Slamon, MD.


Dennis J. Slamon, MD

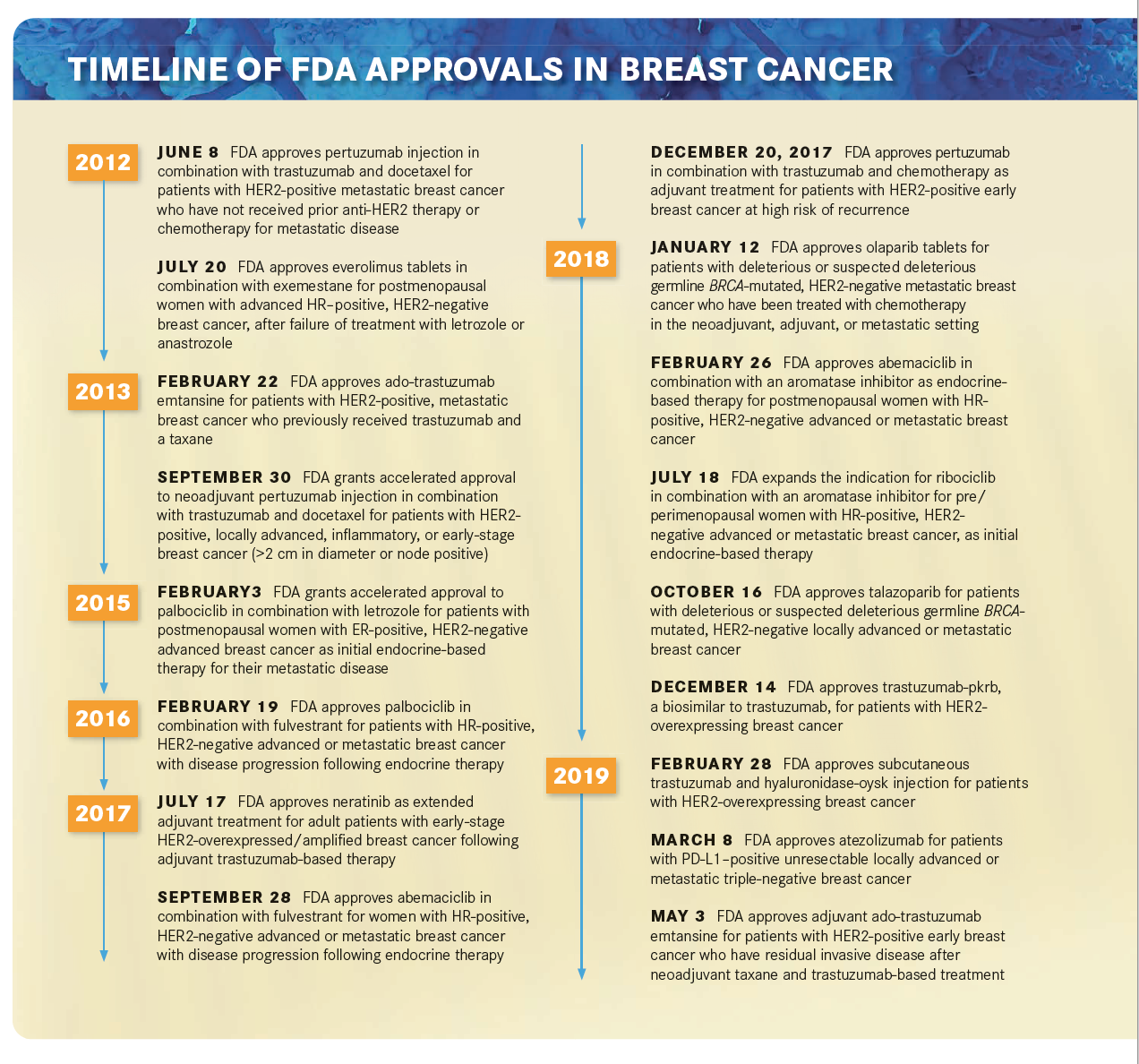
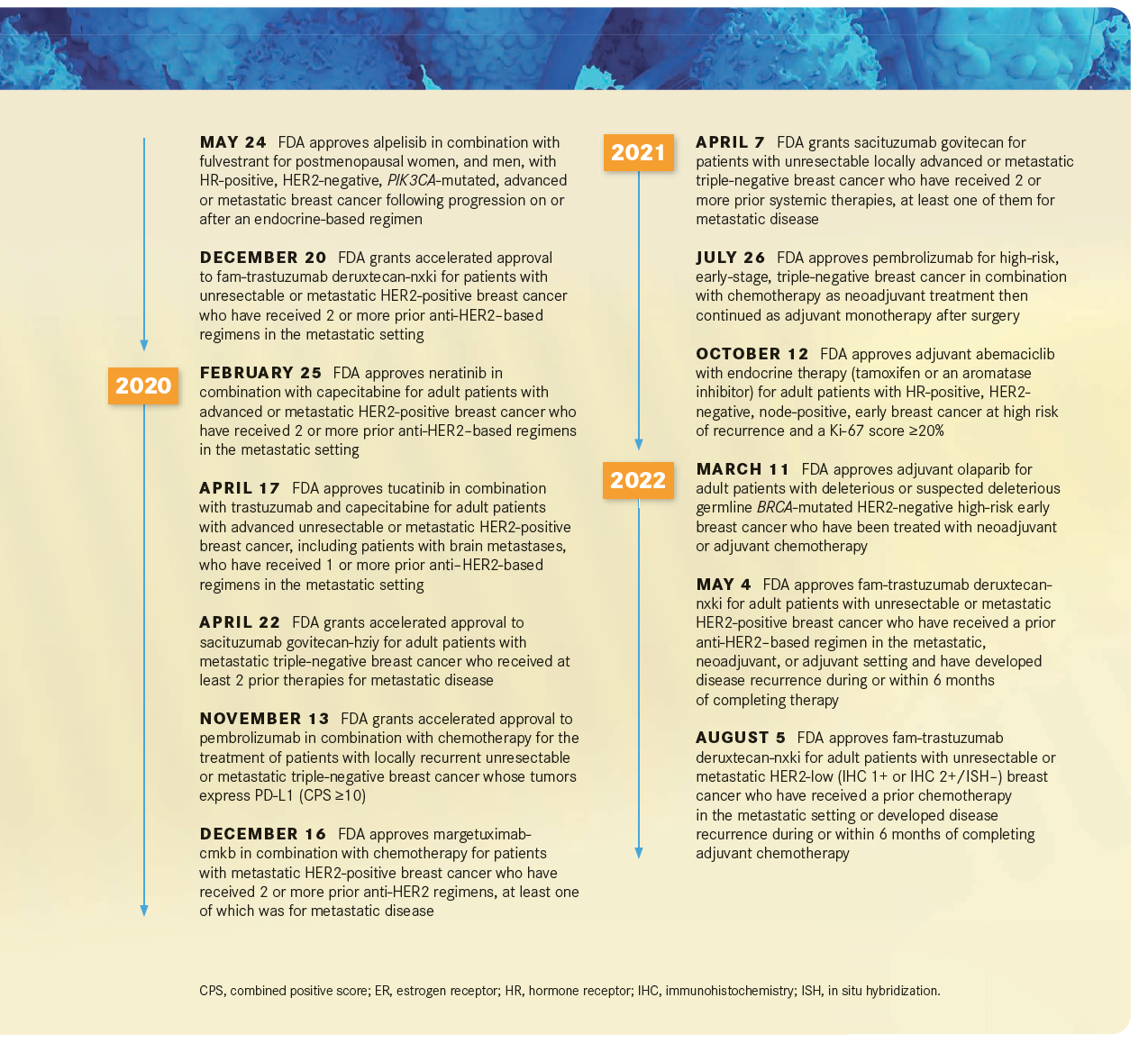
Breast cancer treatment options have significantly expanded in the past decade, welcoming new classes of agents as well as treatments directed at specific patient populations (TIMELINE).
Many believe that these advancements in breast cancer care over the past 10 years owe much to the increased understanding of molecular factors contributing to breast cancer pathogenesis and heterogeneity.1-3
Pushing Molecular Targets Into the Foreground
In looking back at the past decade of targeted therapy in breast cancer, Targeted Therapies in Oncology™ (TTO) spoke with 2 medical oncologists with extensive expertise in breast cancer about how biomarker advancements have transformed the practice of breast cancer management.
“I think it’s fair to say that breast cancer in particular has led the way in molecular therapeutics in oncology,” Dennis J. Slamon, MD, director of clinical/translational research at the UCLA Jonsson Comprehensive Cancer Center, told TTO. “In part, that’s because of all the investment that was made in research [and] because of defi ning this disease not just at a tissue level, but at a molecular level.”
Classification of breast cancers into not just hormone receptor and HER2 positivity or negativity, but also into the luminal/basal subtypes has helped to identify treatments that may be more helpful for large groups of patients.1,3 For example, patients with basal-like disease, which is about 15% to 20% of all breast cancers, have triple-negative breast cancer (TNBC) and a poor prognosis. These patients tend to be responsive to chemotherapy treatment.1
The fact that molecular targets did not consistently translate to all breast cancers has become a key underpinning of our understanding of cancer.1 Not all patients benefi t from molecularly targeted treatments. For instance, HER2-positive breast cancer only accounts for about 25% of all breast cancer cases, thus HER2-targeted therapies may only benefi t 25% of all patients with breast cancer.
“The same story is coming up again and again, not necessarily the same genes or the same targets or the same pathways, but the fact that there is a diversity of these diseases that’s far beyond what we used to use to classify cancers by the tissue in which they arose,” Slamon said.
Early Understanding of Cancer Heterogeneity
Our understanding of cancer as a potentially more complex disease than previously supposed, began to develop well before 2012, explained Slamon.
“That started in breast cancer…before molecular medicine, as far back as 1899 or ’98, when a surgeon recognized the fact that this disease occurred in women and the fact that it may have some hormonal component,” said Slamon.4 “After we found HER2, the methods of dissecting a tumor molecularly became much more sophisticated and widespread in their use and now, today, there are 14 molecular subtypes of breast cancer. And that is the underpinning of how breast cancer has led the way [in determining that patients with breast cancer] should not be treated with a one-size-fits-all approach. They should be treated with therapeutics that are directed to the appropriate subtype or the class in which they sit.”

Marina Sharifi , MD, PhD

These molecular subtype characterizations have also shaped the therapeutic strategies within different breast cancer settings. “Just thinking about advances in targeted therapies and how we use them to treat breast cancer in the last decade, I separate it into 2 categories—1 is how we treat localized breast cancer,when our goal is to cure the cancer, so stages I to III. Most patients are being diagnosed with those earlier stages of breast cancer,” Marina Sharifi , MD, PhD, assistant professor and medical oncologist at the University of Wisconsin Carbone Cancer Center, told TTO.
“I think one of the major themes over the last 10 years for these nonmetastatic breast cancers is what I refer to as right-sizing therapy. We know that some of the women who have these early breast cancers can have recurrence down the road and we want to try and prevent that. So, 10 to 15 years ago, all of those women got chemotherapy, but even back then we knew that not every woman needs chemotherapy, and we knew that there were some breast cancers that could potentially benefit from more targeted types of therapies. But in the past 10 years, there have been a few developments that have allowed us to determine which women need chemotherapy and which women we can safely avoid exposing to the [adverse] effects of chemotherapy,” said Sharifi.
Genomic Testing and Treatment Planning
This new prognostic ability has been fueled by advances in genomic testing.5,6 In addition to hormone receptors and molecular subtypes, other prognostic biomarkers that have been incorporated into practice include transcriptomic and proteomic levels and Ki-67 levels. Other biomarkers utilize combinations of genes to determine potential responses to treatment as well as the possibility of recurrence.

And more recently, research has turned to the use of circulating DNA and circulating tumor cells to help identify further prognostic and predictive bbiomarkers for patients with breast cancer.6
“Specifically, for estrogen-driven (estrogen receptor [ER] positive) breast cancers, which are the most common type of breast cancer, we have genomic tests that are now used routinely to help us identify women who can safely avoid chemotherapy with that type of breast cancer. Both the MammaPrint and the OncoType DX are genomic tests that we know are effective in identifying which women do need chemotherapy to help maximize their chances of cure and which women have lower-risk breast cancers where the chemotherapy actually won’t help them because they don’t need it.7,8 That has been a huge development in the fi eld in the last 10 years—to go from knowing that these tests were out there but not having that confirmation that we know that they predict chemotherapy benefit to having 2 major trials come out in the last 10 years that demonstrate that they can predict chemotherapy benefit, both in women who have those ER-positive breast cancers without lymph node involvement and also women who have ER-positive breast cancer with lymph node involvement. That has been a major advance for the most common type of breast cancer that’s diagnosed across the country.”9,10

Both the TAILORx (NCT00310180) and RxPONDER (NCT01272037) trials validated the usefulness of the 21-gene Oncotype DX recurrence score assay in patients with hormone receptor–positive, HER2-negative breast cancer. The TAILORx trial showed that among patients with node-negative disease, those with an intermediate Oncotype DX score, or intermediate risk of recurrence, could benefit from treatment with endocrine therapy alone and avoid receiving chemotherapy. Younger patients (.50 years) with a recurrence score of 16 to 25 still showed some benefit from the combination of chemotherapy and endocrine therapy.9 I n R xPONDER, adjuvant chemotherapy use was not considered necessary in most postmenopausal women with node-positive disease and recurrence scores between 0 and 25. Alternatively, premenopausal women were more likely to benefit from adjuvant chemotherapy.10
“On the fl ip side,” said Sharifi , “ some…have high-risk TNBC or high-risk HER2-positive breast cancer, those are types of breast cancer where historically we have struggled to cure women. There we’ve had a number of different advances. In TNBC, we’ve had the introduction of immunotherapies into our treatment. The KEYNOTE-522 trial [NCT03036488] showed that if we…combine pembrolizumab [Keytruda] with chemotherapy, that has significantly increased the number of women we’re able to cure of that higher-risk TNBC.”11
Approval of neoadjuvant pembrolizumab in combination with chemotherapy for patients with high-risk, early-stage TNBC followed by single-agent adjuvant pembrolizumab by the FDA in 2021 was a signifi cant advancement for the treatment of patients with TNBC.12 Data from the KEYNOTE-522 trial were considered practice changing early on, showing a pathological complete response in 64.8% of patients treated with the regimen.11
“Likewise, for HER2-positive breast cancer, we have seen the development of multiple drugs that target HER2, from trastuzumab [Herceptin] and pertuzumab [Perjeta], to ado-trastuzumab emtansine [T-DM1; Kadcyla], that have increased the number of women who we’re able to cure of their HER2-positive breast cancers,” Sharifi said.
Slamon also commented on the proliferation of HER2-targeting therapies in addition to the expansion of other types of targeted agents, benefi tting patients in the TNBC space. “[Since] our initial fi nding of HER2 and trastuzumab, now there’s a ton of HER2 targeting— trastuzumab deruxtecan [Enhertu] and emtansine [Kadcyla], margetuximab [Margenza]—the list goes on and on of anti- HER2 therapeutics. Then there are new therapeutics for TNBC; they look at the TROP-2 target on tumor cells, and sacituzumab govitecan [Trodelvy] is the new therapeutic for that.13 As we identify new targets that we can approach with an antibody that’ll attach to it, [it could be possible to] make an antibody- drug conjugate [ADC] to allow that antibody to go right to the target protein on the tumor cell and have it released internally and that takes away the systemic effect of the chemotherapy and delivers it right into the cell. That’s a whole new strategy that’s coming into its own in a big way now,” Slamon told TTO.
The phase 3 ASCENT study (NCT02574455) showed that sacituzumab produced a PFS and overall survival (OS) benefi t over physician’s choice of chemotherapy in patients with relapsed or refractory metastatic TNBC. The median PFS with sacituzumab was 5.6 months compared with 1.7 months with chemotherapy. Median OS was 12.1 months with the ADC and 6.7 months with chemotherapy.13
The emergence of these newer targeted therapies has permitted a risk-based tailoring of neoadjuvant and adjuvant therapies in the non-metastatic breast cancer space, observed Sharifi . “Another major development over the last 10 years, particularly for the [patients with] TNBC and HER2-positive breast cancers, is a shift towards neoadjuvant chemotherapy, which allows us to identify women with higher risk of recurrence after our standard pre-operative chemotherapy, and then add additional therapy after surgery to reduce their risk. For instance, that is how ado-trastuzumab emtansine is used in HER2-positive breast cancer, and there are other targeted options in this space, including olaparib [Lynparza] for women with germline BRCA mutations,” she said.
Metastatic Breast Cancer Advancements
“We have also made great strides in precision oncology in the metastatic breast cancer space, with an expansion of different types of targeted approaches, including mutation-targeted inhibitors, immunotherapy, and ADCs. While all of these developments have helped patients live longer and better with metastatic breast cancer, I think ADCs are the most game-changing new development for treating metastatic breast cancer,” Sharifi told TTO. “As an example, the ADC trastuzumab deruxtecan, is a HER2-targeting agent [encompassing] trastuzumab linked to a chemotherapy that was initially found to be extremely effective for HER2-positive metastatic breast cancer, even in women who have had multiple prior treatments with different other agents. Even more importantly, however, it has recently been shown to be effective also in women who have low HER2 expression, who would previously have been classifi ed as HER2 negative.14 This has dramatically expanded the group of women with metastatic breast cancer who can benefit from trastuzumab deruxtecan to include what we are now calling HER2-low breast cancers, which are far more common than HER2-positive breast cancers. So that’s been an important advance for us in the ADC space just in the last year,” said Sharifi.
Data from the phase 3 DESTINY-Breast04 trial (NCT03734029) showed that patients with low HER2 expression can still possibly benefit from HER2-targeted therapy. The trial demonstrated a median progression-free survival (PFS) of 10.1 months with trastuzumab deruxtecan therapy vs 5.4 months with physician’s choice of therapy in patients with HER2-low (IHC 1+/IHC 2+, ISH-) metastatic breast cancer who had received 1 to 2 prior lines of chemotherapy. The median OS was 23.9 months with trastuzumab deruxtecan and 17.5 months with physician’s choice of chemotherapy.14 These findings led to the FDA approval of trastuzumab deruxtecan in this disease setting just this year.15
The Importance of Individualization
“Turning to mutation-targeted therapies, this has also been an active area in metastatic breast cancer treatment in the past 5 years, including the first FDA approval of a drug targeting PIK3CA mutations, [which] are common in many types of cancer and found in almost half of women who have ER-positive metastatic breast cancer, where the drug alpelisib [Piqray] has been approved for women with this type of mutation,” Sharifi told TTO.
Approval for alpelisib in breast cancer was supported by fi ndings from the phase 3 SOLAR-1 trial (NCT02437318), which showed that the PI3Kα inhibitor in combination with fulvestrant led to a median PFS of 11.0 months vs 5.7 months with fulvestrant in patients with PIK3CA-mutant, HR-positive, HER2-negative advanced breast cancer.16
patient with metastatic breast cancer should be getting molecular profi ling to identify possible targeted therapy options, and many patients will now have ADC treatment options that they may be eligible for at some point in their disease trajectory. For patients with localized breast cancer, I think we’ve also come a long way in being able to individualize therapy and avoid exposing patients to unnecessary [adverse] effects while also being able to augment treatment for patients who are at higher risk of recurrence and cure more women with this diagnosis,” Sharifi said.
The basis of this personalized therapy derived from breast cancer-based research, observed Slamon. “The gamechanger clearly was [the molecular advancements]. [When] looking at what is big in oncology, it’s this appreciation that originated in breast cancer and now has spread throughout the field of human oncology about this molecular diversity defining, a) different subtypes, and b) new potential therapeutic targets or pathways,” he said.
The Future of Breast Cancer Management
Sharifi looks to the continued development of ADCs as a cancer treatment modality. “There’s a real untapped well of potential targets that we’re just starting to explore in terms of developing new ADCs and combining them with targeted and immunotherapy approaches, and I think this will move the bar in how we’re able to combat treatment resistance,” said Sharifi.
Slamon’s view of the future also comprises targeted strategies : “As we identify more targets...there’ll probably be more and newer, perhaps even better, therapeutics than we have currently. Breast cancer has led this field.
REFERENCES:
1. Bettaieb A, Paul C, Plenchette S, Shan J, Chouchane L, Ghiringhelli F. Precision medicine in breast cancer: reality or utopia? J Transl Med. 2017;15(1):139. doi:10.1186/s12967-017-1239-z
2. Cocco S, Piezzo M, Calabrese A, et al. Biomarkers in triple-negative breast cancer: state-of-the-art and future perspectives. Int J Mol Sci. 2020;21(13):4579. doi:10.3390/ijms21134579
3. Low SK, Zembutsu H, Nakamura Y. Breast cancer: The translation of big genomic data to cancer precision medicine. Cancer Sci. 2018;109(3):497-506. doi:10.1111/cas.13463
4. Beatson GT. On the treatment of inoperable cases of carcinoma of the mamma: suggestions for a new method of treatment, with illustrative cases. Trans Med Chir Soc Edinb. 1896;15:153-179.
5. Hou Y, Peng Y, Li Z. Update on prognostic and predictive biomarkers of breast cancer. Semin Diagn Pathol. 2022;39(5):322-332. doi:10.1053/j.semdp.2022.06.015
6. Nicolini A, Ferrari P, Duff y MJ. Prognostic and predictive biomarkers in breast cancer: past, present and future. Semin Cancer Biol. 2018;52(Pt 1):56-73. doi:10.1016/j.semcancer.2017.08.010
7. Cardoso F, van’t Veer LJ, Bogaerts J, et al; MINDACT Investigators. 70- gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016;375(8):717-729. doi:10.1056/NEJMoa1602253






















