Telehealth Delivers Access to Care and Cutting-Edge Clinical Research to Rural Areas
The present and future benefits of telehealth in oncology can be observed through Tahoe For­est Cancer Center and its affiliation with the UC Davis Cancer Center, use of other remote clinics, and participation in virtual tumor boards. Even though there are roadblocks to telehealth reaching more locations and more patients, the potential benefit warrants the time needed to get over those hurdles.



After 25 yearsat Cedars-Sinai in Los Ange­les, California,Laurence Heifetz, MD, moved to Truckee, California, to “recharge his batteries,” in his words. Relocating to a quieter area meant working at a medical facility without an oncology program.
“I went from a hospital with a thousand beds, with [major cancer centers] right down the street, to a town that had no [oncology] services whatsoever and 100% out-migration of all of our patients with cancer,” Heifetz said in an interview at the Association of Community Cancer Centers (ACCC) 36th National Oncology Conference. “Tahoe Forest Hospi­tal requested that we develop a cancer program, and…we decided [to] address issues that were relevant to patients in a rural area. There were 50,000 people up in the mountains who didn’t have cancer services.”
Heifetz is the founder of the Gene Upshaw Memorial Tahoe Forest Cancer Center, where telehealth is a key resource. During the conference, he described the advantages of remote cancer centers working with larger academic facilities, which can benefit both parties, and how telehealth has made a significant impact.
In 2006, Tahoe Forest Hospital started a rudimentary cancer program. The positive response prompted vol­unteers from the Truckee community to form a cancer advisory council, and a freestanding cancer center officially opened in 2012. Since then, it has provided treatment for the rural community and become a model for telehealth. The center offers ease of access and the opportunity to participate in clinical trials to patients in a rural area.
To bring quality cancer services to patients in Truck­ee and the surrounding area, the Tahoe Forest Cancer Center affiliated with the University of California (UC), Davis, Cancer Care Network in 2008. The smaller center became a part of the larger one’s virtual tumor board.
“That relationship allowed us to demonstrate that the patients would be safe and that they would be getting state-of-the-art [care],” Heifetz said. “After about 10 years, starting from zero, we had not only most of the local patients coming in but [also] 62% of our patients coming from outside of our catchment area.”
Sarah Murawski, MPAS, an assistant in medicine at Vanderbilt University Medical Center in Nashville, Tennessee, who presented with Heifetz at the ACCC meeting on telehealth models, also discussed this during an interview.
“In rural areas, telemedicine increases that access to care,” Murawski said. “A lot of patients have to drive hours and hours to get to visits. [With telemedicine], instead of having to come to the institution every sin­gle day for checkups, patients can get labs at outside facilities, and providers can check in with them at local clinics. They can still be seen by a provider, but maybe not a subspecialist, so [telemedicine is] improving access to those subspecialties where patients might have to drive 3 or 4 hours each way to get to a provider.
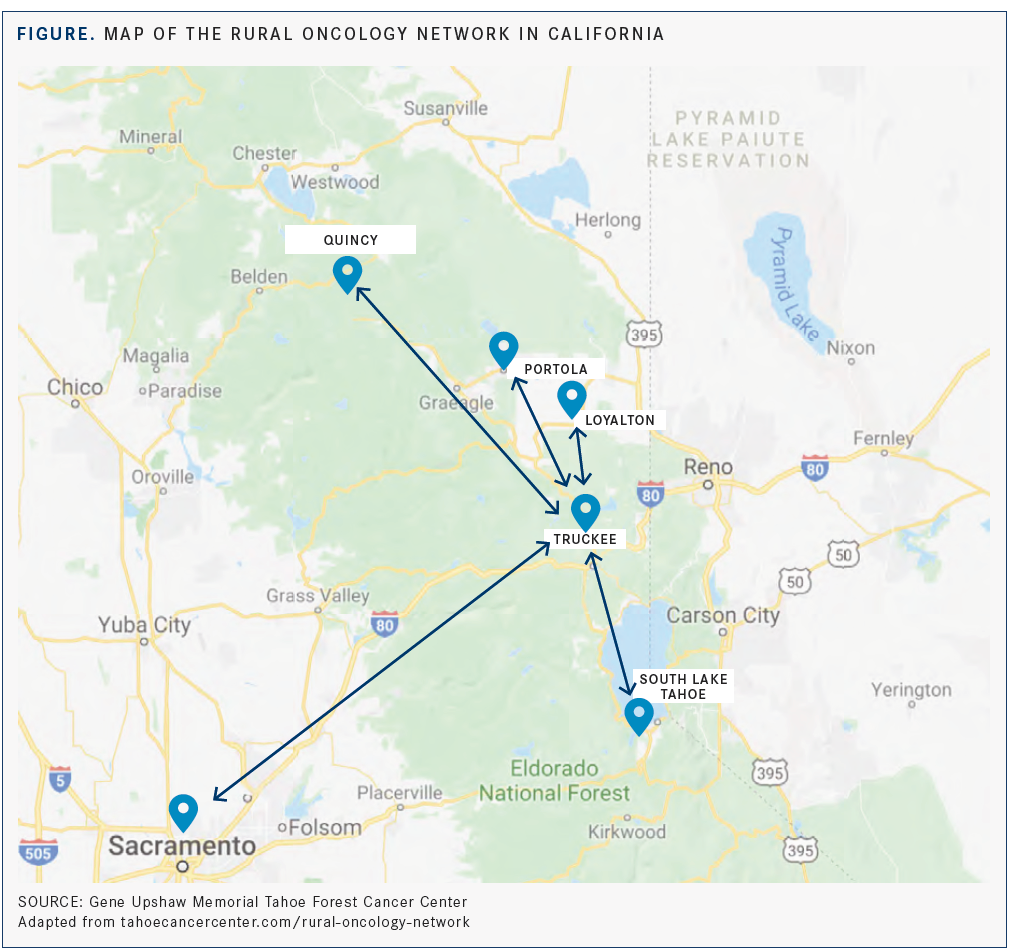
To address this issue, 4 other telemedicine clinics were created in connection with the Tahoe Forest Cancer Center, giving patients access to cancer care in their own communities. These clinics, which make up the Rural Oncology Network, are in Quincy, Portola, Loyalton, and South Lake Tahoe. These clinics include smaller hospitals, some of which were struggling finan­cially, according to Heifetz (FIGURE).
“We can demonstrate a pipeline of knowledge coming from a mother shipthe font of knowledge, which is an academic cancer center—to a remote facility like ours in Lake Tahoe and then going to 4 other, more remote facilities…through our [use] of technology,” he said. “We believe that this is the right way to address dispar­ities in cancer care.”

Even though a patient’s initial visit may be at the Tahoe Forest Cancer Center, subsequent visits can be closer to home. In Heifetz’s opinion, patients prefer seeing a nurse practitioner or physician assistant at their local health­care facility, and having an appointment with an oncolo­gist, whom they already know, through the computer.
“That respects their time, and their buy-in has improved,” he said. “As the patients are feeling more comfortable with being on the [receiving] end of tele­health, the doctors can see the benefit of doing that.”
A cycle of benefits evolved: Because of their affilia­tion with UC Davis Cancer Center, Tahoe Forest Cancer Center gained more people’s trust and brought in more patients. That allowed the smaller center to develop a clinical trials program, which gives UC Davis Cancer Center a percentage of their accrualsthe preferential, advanced cases. The higher accrual rates show the National Cancer Institute that UC Davis Cancer Center has “effective outreach to community oncologists,” Heifetz explained.
Furthermore, Heifetz believes that patients feel more comfortable going to the Tahoe Forest Cancer Center because the physicians are involved in the clinical trials and thus have a better idea of the appropriate treatments. “Clinical trials differentiate if you are practicing at the state-of-the-art [level] or not,” Heifetz said.
Currently, the Tahoe Forest Cancer Center is recruiting for about 30 clinical trials, includ­ing a study combining ipatasertib with atezoli­zumab (Tecentriq) and paclitaxel to treat patients with locally advanced or metastatic triple-negative breast cancer (NCT04177108).
Running clinical trials takes money, so the facility must justify the expense, according to Heifetz. “The justification of that expense is 1 thing only: more patients coming in the door,” he said. “If you see that your combina­tion of clinical trials, your virtual tumor board, and your academic status results in a growth of your program, you know you’re accom­plishing something. In a free market where patients can choose to go to center A versus center B, those are the differentiators that give the patients a sense of security.”
An important part of the collaboration between UC Davis and the remote centers involves the virtual tumors boards. Four days a week, specialists from the UC Davis Cancer Care Network discuss the 4 cancers that affect 80% of their patients. On Mondays the tumor board focuses on gastrointestinal cancers; Tuesdays, genitourinary cancers; Wednesdays, lung cancers; and Thursdays, breast cancers. Network affiliates are Rideout Cancer Center, Mercy UC Davis Cancer Center, the AIS Can­cer Center, Tahoe Forest Cancer Center, and UC Davis Comprehensive Cancer Center.
To become good at [handling] those diseases by participating in virtual tumor boards [means] you’re going to have more patients coming in the door,” Heifetz said.
The virtual tumor boards allow the participating centers to enroll patients in clinical trials faster and more efficiently, and the remote clinics receive more buy-in from their primary care physicians.
Despite the numerous benefits seen with tele­health, legal and financial obstacles exist, and some challenges have no answers just yet.
Heifetz offered the example of sending a patient to a physician outside the state of Cali­fornia: Would that physician seeing the patient remotely need a California license to practice, or would the patient be considered as being seen in the other state?
Providers of telemedicine might need dual licensure to stay within state regulations, Murawski said.
Heifetz posed another question: If the remote appointment takes place inside a hos­pital’s telemedicine office, must the remote physician be a member of that medical staff?
Heifetz and Murawski both touched on finan­cial concerns, with Heifetz citing the issues of billing for a physical examination when the physician can’t touch the patient and how that examination would be carried out.
Technology such as blood pressure cuffs, oxygen monitors, and heart rate monitors aid examinations from afar, inputting data directly into an electronic health record, according to Murawski. She said that the biggest obstacle for many facilities involves reimbursement for the examination and use of these tools. If pro­viders can be reimbursed through private and public insurers, she said, telehealth will be more feasible: Smaller practices can’t always take on those costs, and patients can’t always pay out of pocket.
“I believe those roadblocks are being managed rapidly, and as those roadblocks go away, we’re going to have a much more universal capacity to provide telehealth services,” Heifetz said.
Both Heifetz and Murawski believe tele­health also can play an important role in other areas of oncology. Heifetz sees an opportunity for genetic counseling, which usually doesn’t require a physical exam. He noted the limited number of genetic counselors, whose services are important in the oncology community.
“Down the road, I think social work [could benefit],” Murawski said. “It would be an easy way for [social workers] to do a checkup to make sure patients are getting all the support­ive care that they need. Psycho-oncology is an opportunity to do a virtual support group, so patients don’t have to travel long distances. I think it’s endless, what telemedicine could do for our patients with cancer.”
The present and future benefits of telehealth in oncology can be observed through Tahoe For­est Cancer Center and its affiliation with the UC Davis Cancer Center, use of other remote clinics, and participation in virtual tumor boards. Even though there are roadblocks to telehealth reaching more locations and more patients, the potential benefit warrants the time needed to get over those hurdles.
“I think telehealth is the key to success in a small community practice...the more you can make it easy on your patient to stay close to home, the better your practice is going to sur­vive,” Heifetz concluded.
Reference:
Turgon J, Heifetz L, Murawski S. Telehealth models. Presented at: Associ­ation of Community Cancer Centers 36th National Oncology Conference; October 30-November 1; Orlando, FL

















