Li Reviews Tolerability of Lenvatinib for Advanced HCC
In Partnership With



Daneng Li, MD

Case Summary:
- A 57-year-old woman presented to her primary care physician complaining of abdominal pain and fatigue.
- She had a history of cirrhosis due to heavy alcohol use; Crohn disease, controlled with infliximab; and a history of variceal bleeding, with banding 2 months ago. She has been treated with antiviral therapy for a chronic hepatitis B virus infection for the past 10 years.
- Physical examination showed mild icterus (jaundice) and hepatomegaly. There were no signs of ascites or hepatic encephalopathy. Her ECOG performance status was 1. A CT scan of chest, abdomen, and pelvis with triphasic liver evaluation showed a 4.5-cm LR5 hepatic mass in the right lobe plus metastatic disease in the lung. Laboratory findings included alanine aminotransferase of 68 U/L; aspartate aminotransferase of 70 U/L; total bilirubin 2.6 mg/dL; serum albumin 3.9 g/dL; international normalized ratio of 2.2; α-fetoprotein of 480 ng/mL; hepatitis B surface antigen positive; hepatitis B e antigen negative; and hepatitis B viral DNA (viral load, 1.5 × 105 IU/mL).
- She received a diagnosis of hepatocellular carcinoma (HCC), stage IV, classified as Child-Pugh B7. The biopsy of the liver mass confirmed the HCC diagnosis. Due to autoimmune disease, a nonimmunotherapy was chosen, and she received 12 mg lenvatinib (Lenvima) daily.
- The patient experienced modest weight loss and reported loss of appetite, leading to a dose reduction to 8 mg daily, and she was referred for nutritional therapy. Imaging at 16 weeks showed a partial response. Eight months after initiation of therapy, treatment was discontinued due to disease progression.
Discussion Questions:



• How do the toxicity profiles of lenvatinib and sorafenib (Nexavar) differ as used for unresectable HCC?
• What is your approach to adverse event (AE) prevention, monitoring, and management with each of these agents?
LI: What has been your experience with lenvatinib, and what has been your approach in terms of AE management?
LIU: I have used lenvatinib in different malignancies. I notice the AEs are fairly manageable. Usually with dose reduction, most patients do well. Some people can even tolerate a higher dose, like 14 mg daily. I [am] conscientious; starting low and pushing up is how I usually deal with it.
LI: That’s a great point. Will you usually dose reduce up front in patients with HCC? The lenvatinib dosing for patients with HCC compared with other malignancies is a little bit lower in terms of starting dose.1 Do you further dose reduce even for those patients?
LIU: For HCC, I usually don’t because the dose is low to begin with, but for some other malignancies where the starting dose is 20 mg, I usually start at 14 mg, and then push up.
KOKO: For my experience with lenvatinib, although I start with 8 mg, I’ve always needed to dose reduce. Most of the patients will complain of weight loss and loss of appetite, so I’ve had to hold and then reduce the dose. But otherwise, it’s been fairly well tolerated. I haven’t used sorafenib in ages, though.
LI: What you bring up is a very good point. Our patients with HCC are definitely more vulnerable. It’s a trade-off in terms of AEs compared with sorafenib. With lenvatinib you have less hand-foot-skin reactions, more hypertension, but like you said, potentially more in terms of appetite loss and weight loss. You might [need] that dose reduction for further mitigation.
MAHAJAN: In general, I find it more difficult. We have more experience in using it in combination with pembrolizumab [Keytruda] for renal cell carcinoma and endometrial cancer. It’s a difficult tyrosine kinase inhibitor [TKI]: the hypertension, the skin rash, the proteinuria, the fatigue, so the patients are struggling every day. Every tumor type starts with a different dose. It can be 12 mg, 14 mg, or 20 mg [in other malignancies], so what is the right dose? It may be better compared with sorafenib, which is an equally difficult drug. But compared with immunotherapy and other drugs it’s not easy. It may not be very lethal, but the patients are struggling every day. Especially with diarrhea, skin rash, hand-foot syndrome, proteinuria, and hypertension. You keep going up on the antihypertensive. As a single agent, it may be a bit better, but especially in combination with pembrolizumab in other tumor types, it’s been a challenge.
LI: That’s very well said. I think lenvatinib is a much more potent TKI. This is where AE prevention or AE management is critical. Even with dose reductions, because of the potency of the TKI, it can still get good efficacy as well, so it’s [important to] be cognizant of the AEs and manage the AEs aggressively.
HUANG: With metastatic disease where there is palliative intent of treatment, patient quality of life is more important to me. Most patients I treat with lenvatinib get weight loss and appetite loss, and they couldn’t bear it as an everyday thing. Their quality of life dropped significantly, so I have to dose reduce. I agree that initially, I have to use a lower dose and then try to titrate up, but most of the time I find I have to hold the drug and wait until they get better and then dose reduce further.
LI: I agree that [we need] close monitoring, and if you need to hold the medication and dose reduce, then you [should] do that as well. As you’ve highlighted in terms of focusing on the patient’s experience and their quality of life, some of my patients, even with significant dose reduction, have still been able to be maintained with good efficacy. I don’t think that should prevent anyone from having to dose reduce if they need it for patients who have these AEs that are impairing their quality of life, because they can still get good tumor control in that setting.
LIU: That’s a very good point. I have 2 patients on the same treatment, [though] not for HCC. One was able to push up to 20 mg [lenvatinib]. The other one, I had to dose reduce to 10 mg. Both of them are [maintaining] a complete response. It doesn’t seem to me that the dose is affecting the efficacy as much as we expected.
LI: That is what Dr Mahajan has highlighted. We don’t know what the right dose for each patient with their individual tumor is, and we don’t have anything predictive at this point in time to say that. Whether you’re in the camp of starting lower and then titrating up and monitoring that to get into a tolerable dose that has good efficacy, or you start at the standard dose and then go down with close monitoring at the beginning, those are both very reasonable approaches. What it’s telling you with this medication is that it is a potent TKI, and therefore it does require close monitoring, especially in the very beginning, so that you can make those dose modifications relatively quickly to get it to a very tolerable level for the patients. After you start a patient on lenvatinib, how soon do you follow up with them? Initially, are you seeing them weekly, every 2 weeks, or every month? What’s your practice?
LIU: I usually have my nurse call them in 2 weeks, and I usually see them on a monthly basis, not that I don’t want to see them more often. I just don’t have the capacity to accommodate that. Our nurses check on them, sometimes weekly, sometimes every 2 weeks, depending on how fragile they are and how reliable they are.


LI: Resources do play a role, depending on your individual practice. If you do have the resources, especially in the first month, to be able to check on them once a week, it allows you to capture a lot of these AEs relatively quickly so that you can make modifications. That’s been my personal experience, but I understand that everyone’s resources are very different.
JABBOUR: I have a nurse practitioner with whom I alternate patients who we see together. I’m not a fan of lenvatinib because all of my patients have AEs, but in the first month I alternate with my nurse practitioner. I see the patient one week and the nurse practitioner sees them the other week. We should check the blood pressure, and we should be monitoring the AEs to capture it early.
LI: These are some interesting data in terms of additional realworld data of atezolizumab plus bevacizumab vs lenvatinib in [patients with] Child-Pugh B unresectable [disease]. In this retrospective analysis, all patients received lenvatinib until atezolizumab plus bevacizumab was approved, then, based off a physician choice, but they had the option to remain on lenvatinib or switch to atezolizumab/bevacizumab. So overall, 217 patients were included in this analysis; 65 received atezolizumab plus bevacizumab and 152 or 70% received lenvatinib.
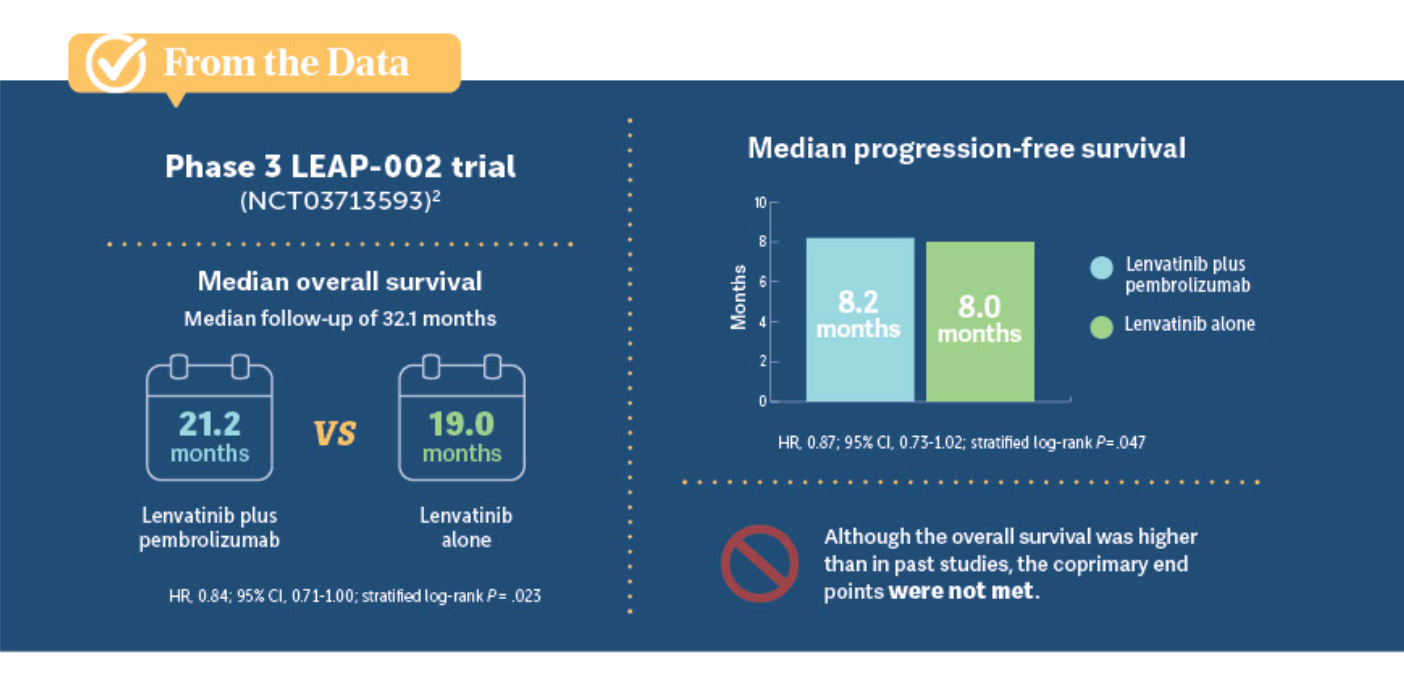
DISCUSSION QUESTION: What were your reactions to the data from the REFLECT (NCT01761266) and LEAP-002 (NCT03713593) trials?
LI: Were you at all familiar with the data for single-agent lenvatinib in the REFLECT trial, as well as some of the other additional analysis that’s been done? In the past year, there were also data from the LEAP-002 study, which compared lenvatinib plus pembrolizumab vs lenvatinib alone.
BADDI: …It’s good to see that there is an option that’s not an immunotherapy, because there seems to be a fair number of patients who have some reason why they cannot tolerate an immunotherapy.... I would just say that one of the more practical issues with this drug is that because it’s oral, it probably results in significantly more financial toxicity for the patient vs the intravenous therapies, which is always a challenge.
LI: Sure, and thank you for highlighting your experience on that. LEAP-002 was a frontline study of lenvatinib plus pembrolizumab vs lenvatinib. Although it was technically a negative study, in the sense that there was no statistical improvement in terms of overall survival between lenvatinib plus pembrolizumab vs the control arm with lenvatinib, the overall survival in that setting for [single-agent lenvatinib] was 19 months, so it was quite high [From the Data2 ]. I think this addresses your point, Dr Baddi, in the sense that some practitioners feel that given this high overall survival that’s very consistent with some of the immunotherapy agents, this gives you a comfortable alternative to consider in the frontline setting.
HUANG: My reaction to REFLECT is that I have started to use lenvatinib more.
LI: Yes, and like I said, it’s good that now we have options in HCC, and [there are] 3 very distinct frontline options to consider for our patients. Options are always good for our patients. I remember when I started in HCC, there was only 1 option that was available, and it was a fairly tough option for our patients.
BADDI: With capecitabine, there were some data that using a diclofenac [topical gel] for the hands helps to reduce the hand-foot syndrome.3 Has that been tested with lenvatinib to see if it’s helpful with this drug as well?
LI: For hand-foot skin reactions I’ve remained with regimens that we’ve used for other TKI-related toxicity, whether it’s clobetasol cream, urea-based creams, [or others]. Usually that’s been able to help manage it, especially when we catch it early on, but we haven’t tested diclofenac that’s been reported with capecitabine. I think that’s a great question to research.

















Advances in Subsequent Therapies Shake Up Sequencing of ccRCC Treatment
April 25th 2024With the approval of belzutifan and other newer data for treating patients with recurrent renal cell carcinoma, the state of subsequent therapies is advancing beyond the reuse of frontline options with impacts on duration of response and quality of life.
Read More

Enhancing Precision in Immunotherapy: CD8 PET-Avidity in RCC
March 1st 2024In this episode of Emerging Experts, Peter Zang, MD, highlights research on baseline CD8 lymph node avidity with 89-Zr-crefmirlimab for the treatment of patients with metastatic renal cell carcinoma and response to immunotherapy.
Listen



Ornstein Advises on Starting Dose and Management of Lenvatinib in RCC
April 21st 2024During a Case-Based Roundtable® event, Moshe Ornstein, MD, MA, provided guidance on dosing and toxicity concerns in a patient treated with lenvatinib plus pembrolizumab for advanced renal cell carcinoma.
Read More

