Updates From the Labs: Taking Skills From Bench to Bedside
A plethora of new technology has been developed to assist in identifying targetable mutations, including next- generation sequencing. NGS assays that identify tumor genes can range in use from targeted to comprehensive panels, all of which have accelerated the advancement of personalized medicine.



Because it has beenwidely accepted that data from tumor samples containing genetic aberrations and oncogenic driver mutations have the potential to improve and personalize patient care, tumor genetic testing is increasingly prevalent in clinical practice.
A plethora of new technology has been developed to assist in identifying targetable mutations, including next-generation sequencing (NGS). NGS assays that identify tumor genes can range in use from targeted to comprehensive panels, all of which have accelerated the advancement of personalized medicine.1
Tumor molecular profiling typically requires tumor tissue biopsy, but some circumstances (eg, patients with metastatic disease) may not allow for adequate sampling. One novel method of molecular profiling includes cell-free DNA (cfDNA), which is derived from circulating blood.
The use of cfDNA is increasing in clinical practice, but this innovative process has some important limitations.2“A regular tumor assay [examines] over 500 genes, and a cell-free assay is a little over 100 genes. When [cfDNA] works, it is great, since it is a noninvasive test to identify mutations, but there are false negatives if there is not enough DNA in the blood or the assay did not cover the mutation,” saidDavid B. Solit, MD, director of Marie-Josée and Henry R. Kravis Center for Molecular Oncology and member of Human Oncology and Pathogenesis Program at Memorial Sloan Kettering Cancer Center in New York.
Actionable Targets
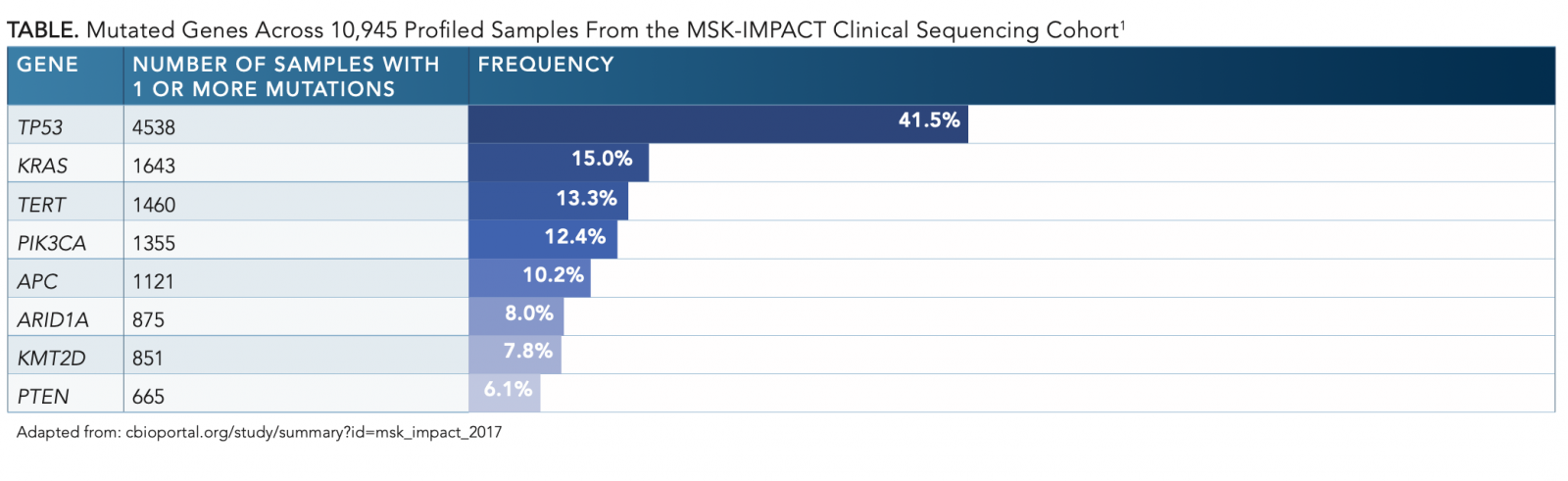
Solit described the NGS assay developed at his institution. Memorial Sloan KetteringIntegrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT) is a prospective genetic testing assay developed and implemented at Memorial Sloan Kettering Cancer Center as a comprehensive NGS panel capable of detecting all protein-coding mutations, DNA copy-number alterations, and other select mutations, such as promoter mutations and structural rearrangements in tumor genes (TABLE).1
Initially, MSK-IMPACT started with the identification of approximately 10,000 patients for tumor gene sequencing in solid tumors and has since “sequenced over 45,000 patients,” with both solid tumors and hematologic malignancies, said Solit. The assay compares tumor cells and normal cells, which “gives an idea why patients may have cancer in the first place [and helps] identify inheritable predisposition mutations likeBRCAmutations,” he explained. MSK-IMPACT was found to be highly consistent with The Cancer Genome Atlas findings in a study by Ahmet Zehir, PhD, and colleagues.1
The tumor types with the highest proportion of mutations for which available therapeutic interventions exist included gastrointestinal stromal tumors, thyroid cancer, breast cancer, and melanoma. Actionable mutations, defined as mutations with matched targeted therapies, were identified in approximately 37% of the tumors tested, and an additional 11% of patients were enrolled in clinical trials for genomically matched tumors.1
Additionally, there were mutations identified that currently do not have a matched targeted drug but are the subject of ongoing research to develop targeted therapies, such asKRAS.1 Solit said that “KRAS[mutations are found] in 15% of cancers, but we do not have inhibitors of KRAS. Development of new treatments againstKRASmutations will be an ongoing effort.” There is insurmountable collaboration between pathologists and oncologists including radiation, surgical, and medical—to “work as a team to interpret [results of the report],” said Solit.
Solit stated that the goal of MSK-IMPACT is to “sequence tumors from all patients with advanced cancer. We are increasingly doing this for patients with earlier-stage cancers, and we use it to guide standard-of-care treatment selection but also to identify patients who might be candidates for clinical trials.”
Solit and his team also use sequencing to “gain insight into novel biology” so they can help identify driver mutations that may cause cancer or disease progression in order to use “sequencing data to identify new drug targets.” Another advantage of MSK-IMPACT is that the program tests all tumor types and can be used for both common and rare cancers, noted Solit.
A study by Pedram Razavi, MD, PhD, and colleagues involved patients with hormone receptorpositive breast cancer. This study helped “identify new methods of resistance to hormone therapy by comparing samples prior to hormonal therapy versus after disease progression on hormonal therapy,” through the implementation of NGS, commented Solit, who was also an investigator on the clinical trial. The data demonstrated that patients withESR1mutations, mitogen-activated protein kinase pathway alterations, or estrogen receptor transcriptional alterations may not respond as well to hormone therapy and should be offered alternative treatment options. These results represent a potential guide to clinical decision making.3Additionally, Solit and his team were able to “identify new resistance byHER2mutations, [which had] not previously been appreciated.”


Using genetic sequencing for all tumor types is important because of the diversity of mutations; however, “there’s better evidence that [genetic sequencing is] more useful in some cancers than others,” said Solit. He noted, “The cancer where it is shown to be the most useful is lung cancer. There are now multiple mutations in lung cancer that guide standard-of- care treatment and experimental treatment.” Genetic sequencing assists clinicians in identifying actionable mutations and detects tumors that may benefit from immunotherapy.
A clinical trial comprising 915 tumors from 860 patients with recurrent or metastatic lung adenocarcinoma with genomic sequencing demonstrated that 37.1% (319/860) of patients received a matched therapy based on the results of their tumor molecular profile with a high likelihood of the mutation predicting a positive response to therapy (P<.001).4Solit stated, “There are more and more options for mutations in some cancer types, like lung cancer withEGFRtumors. We’re starting to see an increasing number of drugs that are better than the older drugs [forEGFR-mutant tumors]. We’re making incremental improvements from some of the drugs we have.”
With the increasing number of targeted therapies directed toward molecular alterations in lung adenocarcinoma, it is the standard of care to retest patients withEGFRmutations after disease progression in order to identify other potentially targetable mutations, such as in “osimertinib [Tagrisso], which will inhibitEGFRT90M gatekeeper mutations,” said Solit.
Unfortunately, not all patients are the beneficiaries of this new approach of precision medicine if tumor types do not have approved matched targeted therapy. For those patients, Solit stated that treatment modalities still include chemotherapy and radiation.
Microsatellite Instability and Tumor Mutational Burden
In addition to genetic mutations, microsatellite instability (MSI) is another biomarker that has garnered interest in the clinical setting. MSI is a condition in which different molecular alterations lead to an impaired mismatch repair (MMR) system and may occur in as many as 24 cancer typescolon and endometrial are the most common. MSI is present in about 5% of all cancer types. Inheritable or sporadic mutations may cause the gain or loss of nucleotides from microsatellite tracts and results in MSI. Tumors with germline or somatic mutations are classified as MMR deficient (dMMR).5
MSI testing identifies patients who may derive benefit from immune checkpoint inhibitors. Testing for MSI may be performed using a commercially available NGS panel or polymerase chain reaction, which is the gold standard for MSI detection. Testing by polymerase chain reaction, and NGS requires samples of tumor and normal tissue, which may not be feasible in some patients. Immunohistochemistry is another test that may be used to determine MSI and MMR status.5
Screening for MSI is quickly becoming the standard of care. MSI-high (MSI-H) tumors are associated with an improved response to immune checkpoint inhibitors and have been a potential biomarker of disease response. Pembrolizumab (Keytruda) was the first drug to be approved by the FDA for patients with MSI-H or dMMR types of solid tumors.5Additionally, nivolumab (Opdivo) with or without ipilimumab (Yervoy) has been FDA approved for the use of MSI-H and dMMR cases of metastatic colorectal cancer.6
Additionally, high tumor mutational burden ( TMB), which represents genomic instability, has the potential to induce neoantigen production and further immunogenicity improvement. TMB is measured by whole-exome sequencing or an NGS cancer gene panel. Similar to MSI, TMB is a potential biomarker predicting response to immune checkpoint inhibitors in cancers including melanoma, lung adenocarcinoma, and urothelial carcinoma.7
TMB can be measured by traditional tissue biopsy or a novel, noninvasive approach using circulating tumor DNA.7 Zhijie Wang, MD, and colleagues demonstrated that patients with high TMB versus low TMB and treated with PD-1 or PD-L1 inhibitors had longer progression-free survival for nonsmall cell lung cancer (HR, 0.36; 95% CI, 0.14-0.93; log- rankP= .03), and the study concluded that TMB as detected in the blood may be a potential predictive biomarker for immunotherapy treatment in this setting.7
Similarly, David R. Gandara, MD, and colleagues also demonstrated that high TMB is associated with an approximately 1-month progression-free survival benefit in the non small cell lung cancer patient population, with a trend favoring the PD-L1 inhibitor atezolizumab ( Tecentriq) compared with docetaxel (HR, 0.57; 95% CI, 0.33-0.99;P= .055).8
There appears to be some overlap with MSI and TMB. Ari VanderWalde, MD, MPH, noticed that in 70% of MSI-H cases, high TMB was also present. However, only 27% of high-TMB cases were identified as MSI-H. The majority of combined MSI-H and high-TMB cases were in colorectal and endometrial cancers. These numbers show that although overlap exists, both MSI and TMB genetic testing should be used to maximize identification of tumors likely to respond to immune checkpoint inhibitors. Additionally, it is unknown whether there are any clinical implications to be derived from the relationship between MSI and TMB status.5
Molecular profiling technology has been used to classify not only solid tumors but hematologic malignancies as well. Testing for mutations in hematologic malignancies is typically performed using flow cytometry, fluorescence in situ hybridization analysis, and/or gene panel testing, such as an NGS assay.9
Genetic sequencing for hematologic malignancies has been used as a prognostic indicator and helps guide treatment, particularly in patients with myeloid malignancies. Additionally, germline mutations inANKRD26,CEBPA,DDX41,GATA2,RUNX1, andSRP72, among others, are associated with familial leukemia disorders.10
One study by Natalie Galanina, MD, and colleagues found that the majority of patients with hematologic cancer had a mutation that corresponded to targeted therapy (75%).11
Molecular profiling is useful in managing patients with hematologic disorders, especially in germline mutations. Patients with high consideration for hematopoietic stem cell therapy with germline mutations are advised to receive stem cells from unrelated donors if family members are also mutation carriers or suspected to be carriers. Otherwise, receiving such stem cells may result in poor engraftment and may potentially lead to donor-derived bone marrow dysfunction.9,12
Patients with myeloid malignancies and germlineCEBPAmutations may require treatment with only chemotherapy because of the long remission periods and favorable outcomes associated with their mutations.12,13Similarly, patients withGATA2mutations may also have favorable outcomes; however, these patients often require anti-microbial prophylaxis against mycobacteria because they are likely to experience frequent atypical infections.9,12,13Furthermore, identifying germline mutations can be critical when managing myeloid malignancies. GermlineRUNX1mutations are associated with early-onset clonal hematopoiesis and cytopenias that may be misdiagnosed as idiopathic thrombocytopenia. Additionally, thrombocytopenia associated withANKRD26is often resistant to corticosteroid therapy and splenectomy.12
Tumor genetic sequencing has shifted the paradigm of cancer treatment to targeted therapy and immunotherapy to match tumor mutations. There is an increasing number of mutations identified through NGS that have already improved cancer care, with multiple novel targeted therapies in clinical trials and in development to target additional identifiable mutations and further advance patient care.
Implementation
Although there is significant benefit seen with molecular sequencing, the implementation process may pose some challenges. Solit noted a few barriers to application, including clinician education, databases, and laboratories providing the interpretation of the results and cost.
“Laboratories [can improve by] providing a report which highlights the actionability of the mutations we find. If the report has a list of mutations, many clinicians [may not] understand which of the mutations are important, [since] they are not trained in interpreting clinical genomic reports,” said Solit. Furthermore, “the report should include information about the mutation and if it is oncogenic and targetable with a drug. These are things that would help clinicians understand [these reports better] because there may be thousands of important mutations, and it would be hard to memorize all that information,” he said.
Solit also called for the development of “databases, which have a link between the mutations and drugs that [target the mutations] to populate the clinical report, [since] one of the challenges is educating clinicians to what these mutations mean and ensure that [they are] interpreting the report correctly so [that patients] can get the right drug.”
“Cost is a problem. Some insurance companies do not pay [for the] testing,” said Solit. However, this can be overcome by “subsidizing the testing through nonprofit support,” he said.
Despite these limitations, molecular profiling of tumors is quickly being used across all cancer centers. Solit said, “Five years ago, [molecular profiling] was not done, but it is now increasingly part of the way we treat [patients with cancer]. This kind of precision personalized care is where oncology is going.”
References
- Zehir A, Benayed R, Shah RH, et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients.Nat Med. 2017;23(6):703-713. doi: 10.1038/ nm.4333.
- Bennett CW, Berchem G, Kim YJ, El-Khoury V. Cell-free DNA and next-generation sequencing in the service of personalized medicine for lung cancer.Oncotarget. 2016;7(43):71013-71035. doi: 10.18632/oncotarget.11717.
- Razavi P, Chang MT, Xu G, et al. The genomic landscape of endocrine-resistant advanced breast cancers.Cancer Cell. 2018;34(3):427-438.e6. doi: 10.1016/j.ccell.2018.08.008.
- Jordan EJ, Kim HR, Arcila ME, et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies.Cancer Discov. 2017;7(6):596-609. doi: 10.1158/2159-8290. CD-16-1337.
- VanderWalde A, Spetzler D, Xiao N, Gatalica Z, Marshall J. Microsatellite instability status determined by next-generation sequencing and compared with PD-L1 and tumor mutational burden in 11,348 patients.Cancer Med. 2018;7(3):746-756. doi: 10.1002/cam4.1372.
- Hematology/oncology (cancer) approvals & safety notifications. FDA website. fda.gov/drugs/resources- information-approved-drugs/hematologyoncology-cancer- approvals-safety-notifications. Updated September 17, 2019. Accessed October 18, 2019.
- Wang Z, Duan J, Cai S, et al. Assessment of blood tumor mutational burden as a potential biomarker for immunotherapy in patients with non-small cell lung cancer with use of a next-generation sequencing cancer gene panel.JAMA Oncol. 2019;5(5):696-702. doi: 10.1001/jamaoncol.2018.7098.
- Gandara DR, Paul SM, Kowanetz M, et al. Blood-based tumor mutational burden as a predictor of clinical benefit in non-small cell lung cancer patients treated with atezolizumab.Nat Med. 2018;24(9):1441-1448. doi: 10.1038/s41591-018-0134-3.
- DiNardo CD, Bannon SA, Routbort M, et al. Evaluation of patients and families with concern for predispositions to hematologic malignancies within the Hereditary Hematologic Malignancy Clinic (HHMC).Clin Lymphoma Myeloma Leuk. 2016;16(7):417-428. doi: 10.1016/j.clml.2016.04.001.
- Godley LA, Shimamura A. Genetic predisposition to hematologic malignancies: management and surveillance.Blood. 2017;130(4):424-432. doi: 10.1182/blood-2017-02-735290.
- Galanina N, Bejar R, Choi M, et al. Comprehensive genomic profiling reveals diverse but actionable molecular portfolios across hematologic malignancies: implications for next generation clinical trials.Cancers (Basel). 2018;11(1):pii:E11. doi: 10.3390/cancers11010011.
- University of Chicago Hematopoietic Malignancies Cancer Risk Team. How I diagnose and manage individuals at risk for inherited myeloid malignancies.Blood. 2016;128(14):1800-1813. doi: 10.1182/blood-2016-05-670240.
- Su L, Tan Y, Lin H, et al. Mutational spectrum of acute myeloid leukemia patients with double CEBPA mutations based on next-generation sequencing and its prognostic significance.Oncotarget. 2018;9(38):24970-24979. doi: 10.18632/ oncotarget.23873.












Priming Agents Show Potential to Improve Liquid Biopsies in Oncology
February 14th 2024In an interview with Targeted Oncology, Shervin Tabrizi, MD, discussed the development of a 2-part priming strategy aimed at enhancing the sensitivity of liquid biopsies for cancer detection and monitoring.
Read More

