Roundtable Roundup: Previously Untreated Multiple Myeloma
In separate live, virtual events, David Dingli, MD, PhD, and Douglas W. Sborov, MD, MS, discussed with participants how they would treat a patient with multiple myeloma in accordance with the available therapeutic regimens.
CASE SUMMARY
A 54-year-old woman presented with Revised International Staging System stage II multiple myeloma, based on evaluations that showed a hemoglobin level of 7.0 g/dL, β2-microglobulin of 6 mg/dL, albumin of 3.2 g/dL, calcium of 11.3 mg/dL, lactate dehydrogenase of 200 U/L, and creatinine clearance of 45 mL/min. Bone marrow showed 22% clonal plasma cells. Serum κ free light chains were 24 mg/dL. She had an ECOG performance score of 1 and no cytogenetic abnormalities. A PET/CT scan showed multiple bone lesions in the vertebrae. She had no extramedullary disease. She was diagnosed with IgGκ myeloma and was considered transplant eligible.




Douglas W. Sborov, MD, MS
Associate Professor
Division of Hematology and Hematologic Malignancies
University of Utah School of Medicine

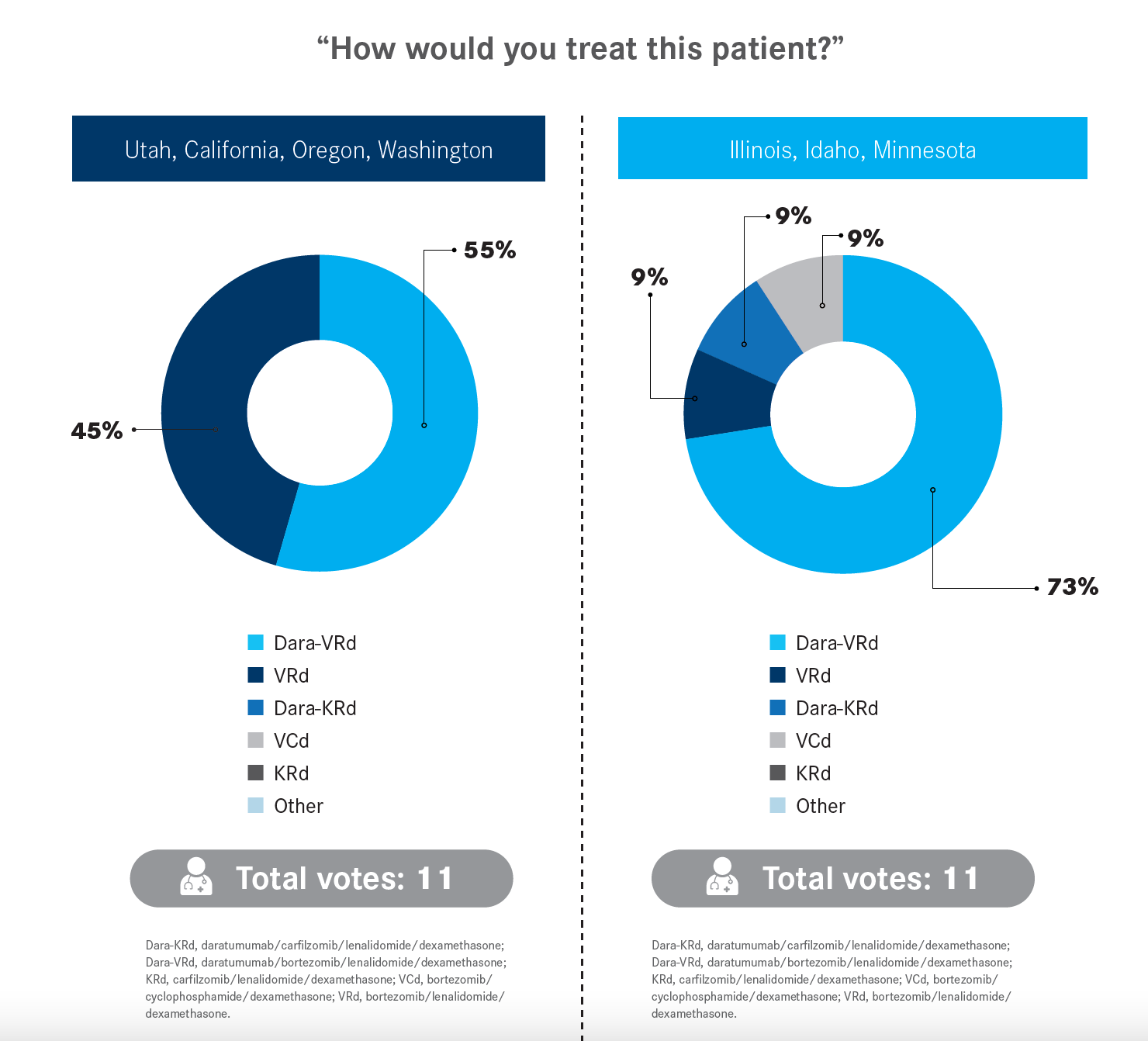
SBOROV: The interesting thing about the polling question here of the quadruplet vs the triplet is it’s very much a debated topic in the newly diagnosed myeloma space right now….We have the newly diagnosed transplant [eligibility] guidelines [from the National Comprehensive Cancer Network (NCCN)].1 VRd [bortezomib (Velcade)/lenalidomide (Revlimid)/dexamethasone] is a preferred regimen; we also include KRd in this [carfilzomib (Kyprolis)/lenalidomide/dexamethasone]. Daratumumab-VRd [is under “other recommended regimens”]….I do want to highlight that we also include Dara-KRd as useful in certain circumstances. If you ever want to move in that direction, you do have the NCCN guidelines to back you up for that quadruplet.

David Dingli, MD, PhD
Professor of Medicine
Mayo Clinic
Rochester, MN

DINGLI: I believe that achieving a deep response in multiple myeloma is very important. The best chance to control the disease and have the longest impact on patients is first-line therapy. If we look at any trial, the longest [progression-free survival] is with first-line therapy. Currently, a patient with newly diagnosed myeloma will be expected to live 8 to 10 years. Half of that or more is based on induction therapy, transplant, and maintenance. A [patient who is] standard risk now is expected to have a response to transplant that could last 50 or 60 months. Well, that’s more than half of their expected survival, assuming there are no developments, which is not [always] the case. But my point is that early decisions are going to have a major impact on the long-term outcome for these patients.
REFERENCES
1. NCCN. Clinical Practice Guidelines in Oncology. Multiple myeloma; version 3.2023. Accessed January 11, 2023. https://bit.ly/2T0mDYS

