ICIs Provide New Treatment Options for Subtypes of Endometrial Cancer
In a presentation during the 39th Annual Chemotherapy Foundation Symposium, Bhavana Pothuri, MD, MS, explained the recent advances in subtypes and treatment options for patients with endometrial cancer.


Bhavana Pothuri, MD, MS

Treatment options for endometrial cancer have evolved over recent years, with significant progress seen in 2021 for treating the distinct molecularly-driven subtypes of endometrial cancer. In a presentation during the 39th Annual Chemotherapy Foundation Symposium (CFS®), Bhavana Pothuri, MD, MS, explained the recent advances in subtypes and treatment options for patients with endometrial cancer.
Moreover, Pothuri added that phase 3 trials of other immune-based combinations with chemotherapy, PARP inhibitors, and other novel agents are on the horizon for 2022 and beyond to target some of these select subsets.
“The endometrial cancer treatment paradigm has changed significantly and will continue to evolve,” said Pothuri, a professor in the Department of Obstetrics and Gynecology and Medicine at NYU Grossman School of Medicine, and director of Gynecologic Oncology Clinical Trials at NYU Langone Health’s Laura & Isaac Perlmutter Cancer Center.
Endometrial cancer is comprised of 4 distinct subtypes: POLE-mutant, microsatellite instability– high (MSI-H)/mismatch repair deficient (dMMR), copy number (CN) low, and CN high/TP53 abnormal. Patients with POLE-mutant disease tend to have the best prognosis compared with CN-low and MSI/dMMR disease (intermediate outcomes), and CN-high/TP53 abnormal disease (worst prognosis).2
Up until 2017, the sole FDA-approved therapy in the endometrial cancer armamentarium was megestrol acetate. Now, clinical practice has benefitted from 3 new regimens that are available based on patients’ molecular profiles: dostarlimab-gxly (Jemperli), pembrolizumab (Keytruda), and pembrolizumab plus lenvatinib (Lenvima).
Recent Regulatory Advances in Endometrial Cancer Treatment
MSI-H/dMMR: Dostarlimab
The multicenter, single-arm, multiple parallel-cohort, open-label, phase 1b GARNET trial (NCT02715284) evaluated single-agent dostarlimab, a PD-1 inhibitor, in expansion cohorts across multiple tumor types, including endometrial cancer. Patients were treated with dostarlimab at 500 mg of intravenous (IV) every 3 weeks for 4 cycles followed by 1000 mg IV every 6 weeks until disease progression.
The trial featured dose-finding (part 1), fixed-dose safety run-in (part 2A), and expansion cohorts (part 2B). In the expansion cohort, there were 5 groups: dMMR endometrial cancer, MMR proficient (pMMR) endometrial cancer, non–small cell lung cancer, nonendometrial dMMR/MSI-H cancer, and platinum-resistant ovarian cancer.
Dostarlimab elicited a 42.3% ORR in 71 patients with dMMR recurrent or advanced endometrial cancer, which included a 12.7% CR rate and a 29.6% PR rate.3 The DOR was at least 6 months for 93.3% of responders, and the median DOR was NR at a median follow-up of 14.1 months (range, 2.6-22.4+).
At a median follow-up of 16.5 months, the ORR via investigator-assessed irRECIST criteria was 45.5% in patients with dMMR endometrial cancer (n = 110).4
Based on the GARNET findings, the FDA granted an accelerated approval in April 2021 to dostarlimab for the treatment of patients with recurrent or advanced endometrial cancer that has progressed on or following prior treatment with a platinum-containing chemotherapy and whose cancers are dMMR, as determined by an FDA-approved test.
The safety profile with dostarlimab was also found to be manageable. Any-grade treatment-emergent AEs (TEAEs) occurred in 69.9% of patients; grade 3 or higher irTRAEs had an incidence of 1.6% or lower. Additionally, increased alanine aminotransferase led to discontinuation in 1.4% of patients, but no TRAEs led to death.
MSI-H/dMMR: Pembrolizumab
The PD-1 inhibitor pembrolizumab was explored in the open-label, nonrandomized, phase 2 KEYNOTE-158 trial (NCT02628067), which comprised previously treated patients with advanced MSI-H/dMMR tumors, including endometrial cancer. Patients received either pembrolizumab at 200 mg every 3 weeks, or at 10 mg/kg every 2 weeks.
Preliminary findings from all-comers showed that the objective response rate (ORR) was 39.6% (95% CI, 31.7%-47.9%), and responses lasting at least 6 months occurred in 78% of responders.5
The FDA granted a tissue-agnostic approval in May 2017 to pembrolizumab based on the preliminary KEYNOTE-158 data, making it the first regulatory approval based on a biomarker regardless of tumor type.
Longer follow-up of the endometrial cancer cohort was presented at the 2021 European Society of Medical Oncology Congress, which had a data cutoff date of October 5, 2020.6 In the efficacy-evaluable population of the endometrial group (cohorts D and K; n = 79), the ORR was 48% (95% CI, 37%-60%), which included a 14% complete response (CR) rate and a 34% partial response rate; 18% of patients had stable disease.
The median time to response was 2.3 months (range, 1.3-10.6). Additionally, the median duration of response (DOR) had not been reached, but 68% of patients were still in response at 3 years. The median progression-free survival (PFS) and overall survival (OS) was 13.1 months (95% CI, 4.3-34.4) and not reached (NR; 95% CI, 27.2-NR), respectively.
Safety with pembrolizumab was consistent with that of other checkpoint inhibitors. Treatment-related adverse events (TRAEs) occurring in at least 10% of patients included pruritus (24%), fatigue (21%), diarrhea (16%), arthralgia (14%), and nausea (14%), hypothyroidism (13%), and rash (11%). Immune-related AEs (irAEs) at any grade occurred in 28% of patients, but 7% of patients experienced these as grade 3/4 events, including colitis (n = 1), severe skin reactions (n = 2), type 1 diabetes mellitus (n = 1), hepatitis (n = 1), and adrenal insuffi ciency (n = 1).
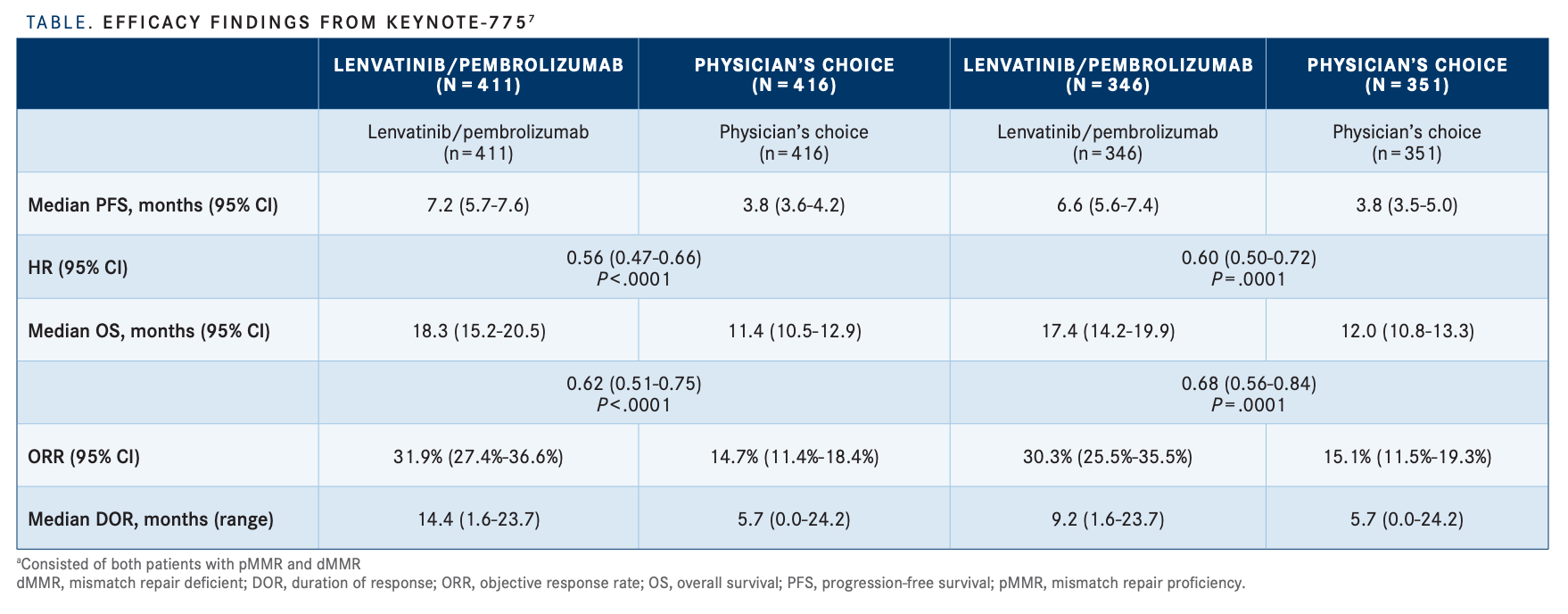
Microsatellite Stable/pMMR: Pembrolizumab/Lenvatinib The combination of pembrolizumab and lenvatinib was tested in patients with advanced endometrial cancer who received prior platinum-based chemotherapy in the phase 3 Study-309/ KEYNOTE-775 trial (NCT03517449).7
At a median follow-up of 11.4 months and in those with microsatellite stable (MSS)/pMMR disease, the median OS was 17.4 months (95% CI, 14.2-19.9) with pembrolizumab/lenvatinib vs 12.0 months (95% CI, 10.8-13.3) with physician’s choice of chemotherapy (HR, 0.68; 95% CI, 0.56-0.84; P < .0001).
Results showed that the median PFS in patients with pMMR status was 6.6 months (95% CI, 5.6-7.4) and 3.8 months (95% CI, 3.6-5.0) with pembrolizumab/lenvatinib and chemotherapy, respectively (HR, 0.60; 95% CI, 0.50-0.72; P < .0001). Here, the ORR was 30.3% (95% CI, 25.5%-35.5%) with pembrolizumab/ lenvatinib vs 15.1% (95% CI, 11.5%-19.3%) with physician’s choice; the median DOR was 9.2 months (range, 1.6-23.7) vs 5.7 months (range, 0.0-24.2), respectively (TABLE).
In all-comers, the median OS was 18.3 months (95% CI, 15.2-20.5) and 11.4 months (95% CI, 10.5-12,9), respectively (HR, 0.62; 95% CI, 0.51-0.75; P < .0001). The median PFS was 7.2 months (95% CI, 5.7-7.6) with pembrolizumab/lenvatinib and 3.8 months (95% CI, 3.6-4.2) with chemotherapy (HR, 0.56; 95% CI, 0.47-0.66; P < .0001). The ORRs were 31.9% (95% CI, 27.4%-36.6%) and 14.7% (95% CI, 11.4%-18.4%) with pembrolizumab/lenvatinib and physician’s choice, respectively. Finally, the median DOR was 14.4 months (range, 1.6-24.2) and 5.7 months (range, 0.0-24.2).
Results of a subgroup analysis from KEYNOTE-775 demonstrated the improvement of pembrolizumab/lenvatinib over physician’s choice of therapy in patients with dMMR endometrial cancer. The median OS with pembrolizumab/lenvatinib-treated patients was NR (95% CI, NR-NR) compared with 8.6 months (95% CI, 5.5-12.9) for physician’s choice of therapy (HR, 0.37; 95% CI, 0.22-0.62; P < .0001).


Here, the median PFS was 10.7 months (95% CI, 5.6-NR) and 3.7 months (95% CI, 3.1-4.4), respectively (HR, 0.36; 95% CI, 0.23- 0.57; P < .0001). The ORRs were 40.0% (95% CI, 28.0%-52.9%) and 12.3% (95% CI, 5.5%- 22.8%), respectively.
The combination was given accelerated approval in September 2019, followed by a regular approval in July 2021, for use in patients with advanced endometrial carcinoma that is not MSI-H/dMMR, who have disease progression following prior systemic therapy in any setting and are ineligible for curative surgery or radiation.
Regarding safety, toxicities associated with pembrolizumab/lenvatinib were consistent with those observed with each therapy given individually. The most frequent all-grade and grade 3 or higher TEAEs included hypertension (64% and 38%, respectively), hypothyroidism (all-grade, 57%), diarrhea (54% and 8%, respectively), nausea (all-grade, 50%), and decreased appetite (45% and 8%, respectively.
Additional grade 3 or higher TEAEs with the combination included weight decrease (10%), anemia (6%), asthenia (6%), fatigue (5%), and proteinuria (5%). It should be noted that 5.7% of patients on pembrolizumab/ lenvatinib died due to grade 5 gastrointestinal disorders (1.2%), cardiac disorders (0.5%), general disorders (1.5%), infections (0.7%), decreased appetite (0.2%), and neoplasms, nervous system, psychiatric, renal, reproductive, or respiratory disorders (0.2% each). This was compared with 4.9% of patients on the physician’s choice arm.
“There are overlapping toxicities to also keep in mind, with the diarrhea and the hypothyroidism. It’s important to sort out: Are those related to the immunotherapy or to the lenvatinib?” Pothuri asked.
Future Biomarker Driven Developments
Ongoing phase 3 trials are tackling more checkpoint inhibitors alone or in combination in endometrial cancer, including RUBY (NCT03981796) with dostarlimab with carboplatin/paclitaxel, RUBY Part 2 with dostarlimab plus niraparib (Zejula; NCT03981796), AtTEnd (NCT03603184) with atezolizumab (Tecentriq), NRGY018 (NCT03914612) with pembrolizumab plus carboplatin/paclitaxel, KEYNOTE-B21 (NCT04634877) with pembrolizumab plus adjuvant chemotherapy with or without radiotherapy, and LEAP-001 (NCT03884101) with pembrolizumab plus lenvatinib.
CN Low
Although CN-low endometrial cancer represents a subgroup of patients that has long been treated with chemotherapy, Pothuri admits that this likely not the optimal approach for this subset, which current research is attempting to confirm.
An additional trial of interest is the phase 2 ENGOT-EN3/NSGO-PALEO study (NCT02730429), which enrolled patients with primary stage IV or relapsed measurable/ evaluable endometrial cancer who have received at least 1 prior systemic therapy. Patients were randomized 1:1 to receive palbociclib (Ibrance) at 125 mg days 1 to 21 plus letrozole at 2.5 mg on days 1 to 28 vs placebo and letrozole at the same dosage schedule every 28 days until disease progression. The primary end point was investigator-assessed PFS.
Data showed that the median PFS was 8.3 months and 3.0 months for the palbociclib/ letrozole and placebo/letrozole arms, respectively (HR, 0.56; 95% CI, 0.32-0.98; P = .0376).8 Additionally, the disease control rate was 63.6% and 37.8%, respectively.
“This was a phase 2 study and needs further study to determine if there is a role of CDK4/6 and hormonal therapy,” Pothuri added.
CN High
Patients with CN-high endometrial cancer form a group that is classically comprised of TP53-positive, high-grade, serous, and ERRB2 positive-tumors, Pothuri explained, adding that homologous recombination deficiency is frequent in this subset and may be actionable.
For example, in a phase 2 trial (NCT01367002), patients with HER2-neu uterine serous carcinoma were randomized to receive carboplatin/paclitaxel for 6 cycles with or without IV trastuzumab (Herceptin) until progression or unacceptable toxicity. Data showed that in all patients the median PFS was 12.6 months with the addition of trastuzumab vs 8.0 months for carboplatin/ paclitaxel alone (HR, 0.44; 90% CI, 0.26-0.76; P = .005).9 In those with primary stage III to IV disease, the median PFS was 17.9 months and 9.3 months, respectively (HR, 0.40; 90% CI, 0.20-0.80; one-sided P = .013). In recurrent disease, the median PFS was 9.2 months and 6.0 months, respectively (HR, 0.14; 90% CI, 0.04-0.53; P = .003).
An updated analysis showed an OS benefit in the stage III to IV subgroup, in which the median OS was NR in the trastuzumab arm vs 25.4 months with chemotherapy alone (HR, 0.49; 90% CI, 0.25-0.97; P = .041).10
“[There is] lots of great interest, and it is really an exciting time to be in the endometrial cancer space,” Pothuri said. “The role of trastuzumab and other HER2/neu-directed therapies for CN-high biomarker-positive tumors also needs further investigation in phase 3 trials.”
REFERENCES
1. Pothuri B. Biomarker driven management of endometrial cancer. Presented at: 39th Annual CFS®: November 3-5, 2021; New York, NY.
2. Levine DA,The Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67-73. doi:10.1038/nature12113
3. Oaknin A, Tinker AV, Gilbert L, et al. Clinical activity and safety of the anti–programmed death 1 monoclonal antibody dostarlimab for patients with recurrent or advanced mismatch repair–defi cient endometrial cancer: a nonrandomized phase 1 clinical trial. JAMA Oncol. 2020;6(11):1766-1772. doi:10.1001/jamaoncol.2020.4515
4. Oaknin A, Gilbert L, Tinker AV, et al. Interim analysis of the immune-related endpoints of the mismatch repair defi cient (dMMR) and profi cient (MMRp) endometrial cancer cohorts from the GARNET study. Gyn Oncol. 2021;162(suppl 1):S12-S13. doi:10.1016/S0090- 8258(21)00672-7
5. FDA grants accelerated approval to pembrolizumab for fi rst tissue/ site agnostic indication. FDA. May 23, 2017. Accessed November 4, 2021. https://bit.ly/3k62CMS
6. O’Malley DM, Bariani GM, Cassier PA, et al. Pembrolizumab (pembro) in patients (pts) with microsatellite instability-high (MSI-H) advanced endometrial cancer (EC): Updated results from KEYNOTE-158. Ann Oncol. 2021;32(suppl_5):S725-S772. doi:10.1016/annonc/ annonc703
7. Makker V, Colombo N, Herráez AC, et al. A multicenter, open-label, randomized, phase 3 study to compare the efficacy and safety of lenvatinib in combination with pembrolizumab vs treatment of physician’s choice in patients with advanced endometrial cancer: Study 309/KEYNOTE-775. Gyn Oncol. 2021;162(suppl 1):S4. doi:10.1016/ S0090-8258(21)00657-0
8. Mirza MR, BjørgeL, Marmé F, et al. A randomised double-blind placebo-controlled phase II trial of palbociclib combined with letrozole (L) in patients (pts) with oestrogen receptor-positive (ER+) advanced/ recurrent endometrial cancer (EC): NSGO-PALEO / ENGOT-EN3 trial. Ann Oncol. 2020;31(suppl_4):S1142-S1215. doi:10.1016/annonc/ annonc325
9. Fader AN, Roque DM, Siegel E, et al. Randomized phase II trial of carboplatin-paclitaxel versus carboplatin-paclitaxel-trastuzumab in uterine serous carcinomas that overexpress human epidermal growth factor receptor 2/neu. J Clin Oncol. 2018;36(20):2044-2051. doi:10.1200/JCO.2017.76.5966
10. Fader AN, Roque DM, Siegel E, et al. Randomized phase II trial of carboplatin-paclitaxel compared with carboplatin-paclitaxel-trastuzumab in advanced (stage III-IV) or recurrent uterine serous carcinomas that overexpress her2/neu (NCT01367002): updated overall survival analysis. Clin Cancer Res. 2020;26(15):3928-3935. doi:10.1158/1078-0432.CCR-20-0953








Survivorship Care Promotes Evidence-Based Approaches for Quality of Life and Beyond
March 21st 2025Frank J. Penedo, PhD, explains the challenges of survivorship care for patients with cancer and how he implements programs to support patients’ emotional, physical, and practical needs.
Read More






