Experts Address Breast Cancer Relapse on AI Therapy During Targeted Tweet Chat
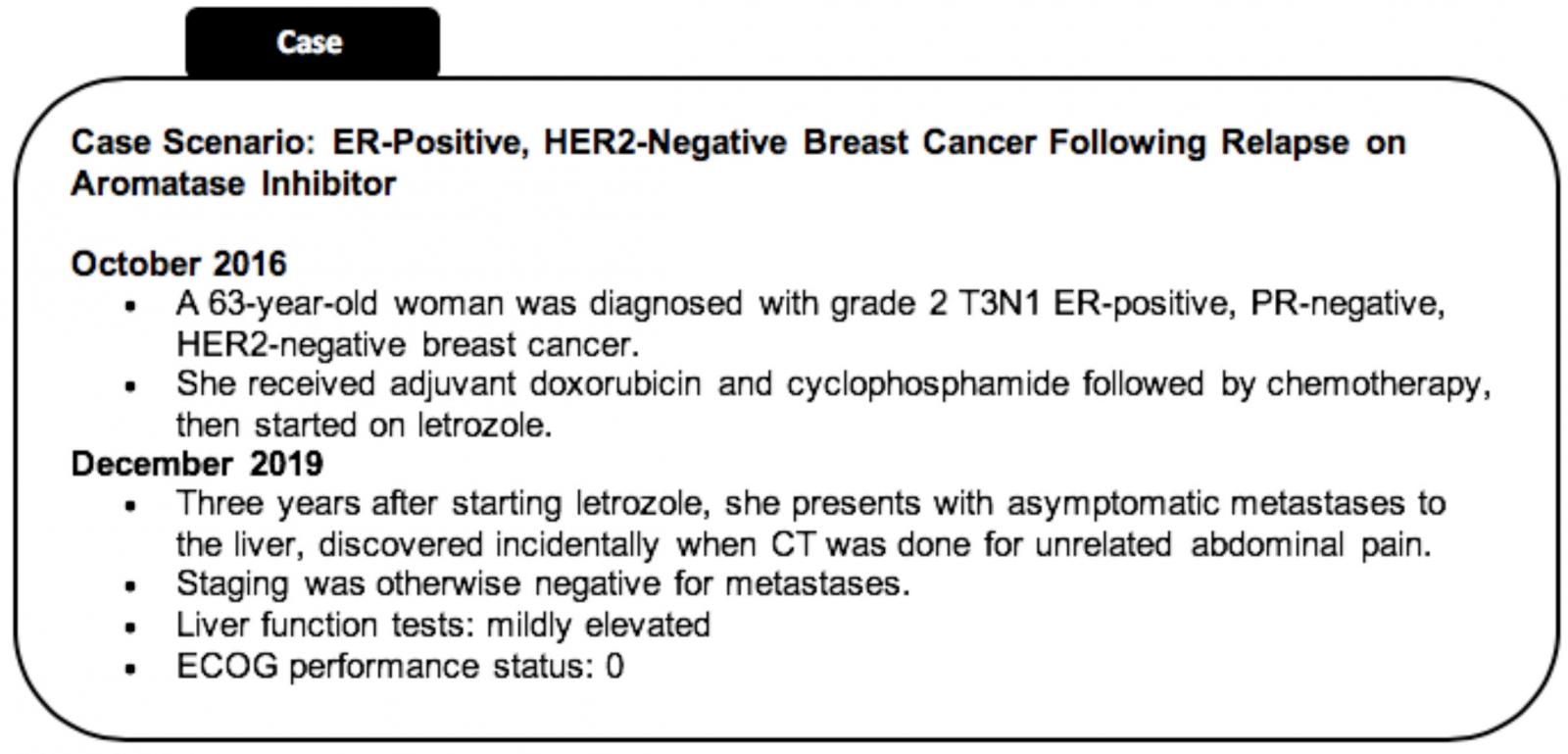
During a Targeted Oncology tweet chat, Erika P. Hamilton, MD, and Stephanie Graff, MD, discussed treatment options and considerations for the case of a patient with ER-positive, HER2-negative breast cancer who relapsed on letrozole, an aromatase inhibitor.


Erika P. Hamilton, MD

Erika P. Hamilton, MD
During aTargeted Oncologytweet chat, Erika P. Hamilton, MD, director of the breast cancer and gynecologic cancer research program, and Stephanie Graff, MD, associate director of the breast cancer research program at Sarah Cannon Research Institute, discussed treatment options and considerations for the case of a patient with estrogen receptor (ER)-positive, HER2-negative breast cancer who relapsed on letrozole (Femara), an aromatase inhibitor (AI). They reviewed the options from a Twitter poll and how they would approach treatment for this particular patient.




Stephanie Graff, MD

Stephanie Graff, MD
A Twitter poll ahead of the tweet chat asked which of 4 options would be the next best line of therapy for this patient case. Choices included chemotherapy, CDK4/6 inhibition plus fulvestrant (Faslodex), CDK4/6 plus AI, and hormonal therapy as a single agent. The vote favored CDK4/6 inhibition with fulvestrant by roughly 91.3%, which both Graff and Hamilton agreed with.
Three CDK4/6 inhibitors are currently approved by the FDA, including palbociclib (Ibrance), abemaciclib (Verzenio), and ribociclib (Kisqali). These different agents have demonstrated similar clinical benefit in trials, so Graff and Hamilton agreed that the choice of the appropriate CDK/6 inhibitor for the patient should come down to the toxicity profiles associated with each agent, as well as what the treating physician is comfortable with using.
CDK4/6 inhibitors can be combined with either an AI or fulvestrant, but our experts were in agreement that for this patient case, the backbone of AI therapy should be switched to fulvestrant due to relapse while on the AI. Should the patient relapse again following CDK4/6 inhibition plus fulvestrant, both experts recommend more genetic testing to determine the next best line of therapy, which could include clinical trial.
Hard questions! So unfortunately many agents are combined with fulvestrant. So, for someone who progressed on CDK4/6+fulvestrant we don’t know the role of alpelisib. But with so many targeted agents in development you need to look at trial options.#TargetedCaseChat
Stephanie Graff, MD, FACP (@DrSGraff)December 19, 2019
Hamilton favors the idea of treating this patient with a selective estrogen receptor degrader (SERD) on a clinical trial. SERDs have demonstrated tolerability in patients with breast cancer and are administered orally, so patients can take the medication at home as opposed to in a hospital intravenously, says Hamilton.
In an interview withTargeted Oncologyfollowing the tweet chat, Hamilton reviewed key discussion points from this patient case and her rationale for selecting a CDK4/6 inhibitor in combination with fulvestrant. She also highlighted the role of genetic testing in patients with breast cancer and important considerations when making treatment decisions in breast cancer.
TARGETED ONCOLOGY: What factors would you consider while making your decision for this particular patient case?
Hamilton:There are a variety of things to take into consideration for this patient case. For the patient who has relapsed while on an AI, I would want to see what duration of benefit they had from that. The only thing we truly have as a predictor to not get benefit out of a CDK4/6 inhibitor is to not be ER-driven. Often, if somebody is newly relapsed or there has been some time since they have had a biopsy, this is when we would go back in, get a small piece of tissue, and make sure their cancer is still strongly HR-positive.
I would also take into account the patient’s baseline conditions. We got into this a little bit in the tweet chat, but the agents are a little different in terms of gastrointestinal (GI) side effects and neutropenia. For somebody who runs a low white blood cell, abemaciclib, for example, might be a nice option, or for somebody who has constipation at baseline due to pain medications, abemaciclib might be a nice treatment as well, compared with somebody who is worried about diarrhea from day-to-day activity. That patient would be a nice candidate for palbociclib or ribociclib to avoid diarrhea.
TARGETED ONCOLOGY: The results from our poll clearly favored the combination of CDK4/6 inhibition with fulvestrant. What is your rationale for selecting this treatment option?
Hamilton:Uniformly, everyone would be thinking about a CDK4/6 inhibitor for this patient. The real question comes down to the endocrine backbone, and our choices are either AI or fulvestrant. Because this patient was on an AI when she relapsed, we would change her backbone to fulvestrant and not “reuse” the AI.
We can use AIs in combination with CDK4/6 inhibitors in the first-line setting for patients who are not on an AI when they relapse and have had some time since they went off that medication or do not take it. We would expect them to still be sensitive to an AI.
TARGETED ONCOLOGY: With 3 CDK4/6 inhibitors approved by the FDA, which is most suitable for this patient population?
Hamilton:All the CDK4/6 inhibitors, abemaciclib, ribociclib, and palbociclib, have shown very similar efficacy across the clinical trials. The hazard ratios look almost identical in that 0.5 range. We are hard-pressed to point to the fact that we don’t have evidence 1 works better than the other.
However, there are some differences in the side effects, such as GI disturbance and neutrophil count. Ribociclib also requires live function test monitoring and monitoring of the EKGs. All of these come together to make a decision. Quite honestly, a lot of physicians use the 1 they are most familiar with using or the 1 that they have a preference for. We don’t have any concrete reasons to think 1 CDK4/6 inhibitor works better than the other 2.
TARGETED ONCOLOGY: Should this patient progress after the CDK4/6 inhibitor and fulvestrant, what would be your next best line of therapy?
Hamilton:I would profile this patient. I normally profile patients in the first-line or at least by the second-line setting to see if there are any other drivers in the tumor to identify. Dr. Graff shared a good list during the discussion [tweet below].
I would be thinking about a clinical trial for this patient. We try to exhaust endocrine therapy as long as the patient is still sensitive to endocrine therapy. There are a handful of good oral SERD clinical trials. These are essentially the next-generation of the fulvestrant molecule, but they are pills. Patients don’t have to get a shot, and it’s something they can take at home. They are very well tolerated, so I would be thinking about getting this patient access to an oral SERD.
BRCA, MSI, PDL1/PD1, PI3K, ESR1, ERBB2, and on and on might open up targeted options or clinical trials unique to that particular patient.#TargetedCaseChat
Stephanie Graff, MD, FACP (@DrSGraff)December 19, 2019
TARGETED ONCOLOGY: Dr. Graff emphasized the importance of genetic testing during our tweet chat. Could you discuss how genetic testing at this time could impact treatment selection in this patient case?
Hamilton:One type of genetic testing is for the inheritedBRCA1/2genes. We know patients can have BRCAabnormalities in their tumors that are germline or because they have inherited the gene that predisposed them to breast cancer. We also sometimes see what is called somaticBRCAalterations. That is where the mistake is just in the tumor and is not in the rest of the person. It’s something that the tumor acquired.
We have evidence that germline and somatic mutations respond to PARP inhibitors, and we have 2 approved PARP inhibitors for breast cancer now, including talazoparib (Talzenna) and olaparib (Lynparza). I would be very interested in knowing whether this patient’s tumor harbored aBRCAalteration.
We also have alpelisib, which is a Pi3K inhibitor approved by the FDA. Interestingly, it is approved in combination with fulvestrant, so we typically think of using it in the second-line. For a patient like this who relapsed while on an AI, they would probably be using fulvestrant in the first-line, but alpelisib is definitely a drug we could consider.
It’s rare for patients with hormonally-driven cancers to have markers that would predict benefit to immunotherapies, but if we found something like that, it would certainly be interesting in a clinical trial as well.
We still have everolimus (Afinitor) and exemestane (Aromasin), which is an oldie but goodie combination that is a steroidal AI in combination with an mTOR inhibitor. If we profile this patient and she didn’t have anESR1mutation, then exemestane and everolimus would be a very reasonable option for her. TheESR1mutation predicts resistance to the AIs, but a lot of times, patients continue to be sensitive to SERDs, whether that is fulvestrant or an oral SERD.
These are some of the reasons why, based on what the profile shows, we might tailor an individual patient’s treatment toward 1 direction or another.
TARGETED ONCOLOGY: Now that the tweet chat has ended, what do you hope people take away from the discussion of this patient case?
Hamilton:The biggest thing to take away is that some people are a little resistant to the use of new medications. It takes a while for the word to get out there so that everybody is comfortable using them. I think most people in the United States are comfortable using CDK4/6 inhibitors, but the market data still shows that not every patient is receiving 1. I think the take home point is the dramatic benefit we have seen for those in progression-free survival, as well as overall survival (OS), across all 3 of these agents. With an OS benefit in this hormonally-driven breast cancer that all patients should be receiving a CDK4/6 inhibitor, whether it is in the first-line or second-line. In my practice, I do use a CDK4/6 inhibitor in the first-line, but some people choose to use these it in the second-line instead.
I agree with the voting audience on treatment! CDK4/6 inhibitors have changed the landscape of first line ER+ mBC.#TargetedCaseChat
Stephanie Graff, MD, FACP (@DrSGraff)December 19, 2019














