Dealing With a Patient’s Financial Distress
One of the leading non-clinical attributes that affect how oncologists decide which therapeutic agent to prescribe over another is patient affordability.


Daniel Sherman

Daniel Sherman, MA
One of the leading non-clinical attributes that affect how oncologists decide which therapeutic agent to prescribe over another is patient affordability. As more and more insurance benefit designs shift the costs of treatment to the patient, affordability will continue to grow as a significant factor that contributes to patient adherence.
“I was an oncology social worker for well over 10 years and I found that I was spending most of my time dealing with the patient’s financial distress,” said Daniel Sherman, MA, LPC, a licensed professional counselor. “The number 1 issue was financial.”
To emphasize that point, a recent survey of insured patients who were receiving treatment for breast, lung, or colorectal cancer demonstrated that financial distress and out-of-pocket costs have several consequences for patients: 70% of patients reduced leisure activities, 48% withdrew savings, and 18% sold possessions. This distress also may result in decreased compliance. As many oncologists can attest, the financial distress of cancer care can significantly affect quality of life and treatment compliance.1


How to help patients pay for treatment
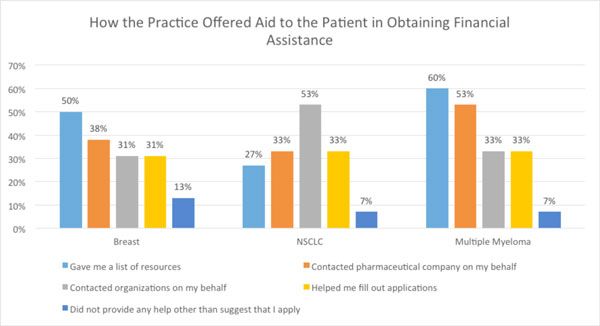
Source: Kantar Health, Patient Survey,
Terms such asfinancial toxicityandfinancial distresswere not part of a typical conversation between oncologist and patient 10 or 15 years ago, said Sherman. But with annual direct costs for cancer care projected to rise from $104 billion in 2006 to over $173 billion in 2020 and beyond, and the increased media attention to the financial burden of cancer care, stakeholders such as oncologists, patients, insurers, and the pharmaceutical industry are looking for ways to ease the financial burden that can accompany a cancer diagnosis.2
Considerations for the Practice
If a practice is considering hiring a financial navigator there are some considerations. “Depending on the size of the practice and number of patients being seen, I would estimate that a full-time financial navigator can see about 800 new cases a year,” said Sherman.
For uninsured patients, navigators can (See Figure)
- Facilitate enrollment in health care exchange plans
- Help patients enroll in Medicaid/Medi-Cal programs
- Apply for social security and disability benefits on behalf of the patient
- Identify and aid the patient to apply for free medications
In many cases, according to Sherman, the biggest obstacle is convincing the practice’s management team that adding another full-time employee (FTE) is needed. He emphasizes that for patients, the main concernafter the fear of dying from the disease—is how am I going to pay for this treatment? “I have found that patients are eager to have this conversation,” he continued. “Especially if there are options to minimize their out-of-pocket responsibilities.”
Navigators can also identify external sources to help pay for treatment, including:
- Foundations
- Pharmaceutical sponsored programs
- Local philanthropic organizations
- Cancer center’s charity program
Hiring a financial navigator has a distinct effect on other employees within the practice, as well. “For the oncologist, it improves access to care for the patient. The nurses are thrilled because it decreases the patient’s distress. Oncology social workers are thrilled because it limits their case load.”
“I think the oncology community has finally caught up and recognizes this as a problem,” said Sherman. There are a number of financial assistance program options that a navigator can explore with his patient. This includes manufacturer-direct programs and programs that aid the underinsured or uninsured patient. Financial assistance programs are evolving and oncology practices place increasing value on them.
“Using patient assistance programs offered by the drug manufacturer can provide a temporary fix,” said Sherman. In addition to alleviating some financial distress, well-designed manufacturer-direct programs help keep prescriber decisions focused on clinical, rather than financial, considerations. “Another source of assistance are programs sponsored by foundations that can help with the patient’s out-of-pocket responsibilities.” Minimizing practice burden should be a key consideration in structuring program access, information, enrollment, and qualification. Developing strategies to support underinsured patients in the state exchanges will be essential to ensure continued access and adherence for this patient population.
For Medicare patients, helping them choose the Medicare plan that provides the best coverage is an important responsibility of the financial navigator. “It’s quite complicated to educate the patient about picking better Medicare plans,” Sherman said. The benefit, though, is that the patient has 100% of coverage and “is under so much less distress than what they were under before financial counseling.” In addition, oncology practices and hospitals aren’t forced to collect copayments or coinsurance from their Medicare patients.
Patient Flow
Sherman points out that not every patient needs a financial navigator. Usually before the first consult, the navigator will review the patient’s insurance benefits package. If he notices a significant out-of-pocket responsibility or if the patient appears to be uninsured or underinsured, these are patients who might benefit from a discussion with a navigator. “It’s typically 25% of all patients who come through the door.”
Sherman would recommend bringing in the financial navigator on the day of the initial consult. “We know that our patients are coming with this concern, on the day of the consult they are concerned with diagnosis and prognosis. They quickly shift to ‘how am I going to pay for this?’ So you catch them immediately. And the earlier the financial navigator can get involved, the easier to find solutions by identifying appropriate aid programs, or educating the patient to choose better insurance. The faster you do this the better it is for the patient.”
In addition, on the day of the consult, “it’s typical that other family members are present as well,” said Sherman. “I love it when the family is present because I’m educating everyone at the same time.” And while educating the patient about the different benefits and plan designs, it might come to light that the patient cannot afford to pay an additional $50 or $100 a month. At this point, another family member, whether it’s a son or daughter, or if it’s the son or daughter with the diagnosis, the parent, might offer to help pay for the added premium. “That removes the financial burden from the discussion and the patient can focus on just receiving the treatment,” he said.
Another consideration is in this age of health reform, patients enrolled in “bronze” health plans have about a $6300 out-of-pocket responsibility says Sherman. “Many patients still don’t know that if they are below 250% of the federal poverty level, they can receive subsidies,” said Sherman. “But this only applies to silver plans. I’ve had patients who say they’ve picked the gold plan, thus reducing their out-of-pocket costs, only to discover that if they had picked a silver plan, they would have had an even smaller deductible because of the subsidies.”
He said, “There are some patients who are much better off because of reform. But there are some who are not better off. The majority are better, especially if they were uninsured.”
With the many advances being made in research and treatment, some types of cancers are being chronically treated. With that comes copayments, coinsurance, and other out-of-pocket expenses for patients. The role of the financial navigator is growing.
“It is a ‘must have’ service within oncology,” said Sherman. “Patients who don’t seek our help can suffer needlessly. There are so many things that can be done to decrease the distress to the patient. Patients are experiencing more financial distress than they have to,” he said.
Oncologists Respond to Financial Toxicity
Unfortunately, along with the distress that comes with a cancer diagnosis and the discomforts of treatment, more patients now have to deal with “financial toxicity,” the expense, anxiety and loss of confidence confronting those who face large, unpredictable costs, often compounded by decreased ability to work. Financial pain may extend beyond treatment. A recent study from the Centers for Disease Control and Prevention found that 30% of cancer survivors are not able to return to work, or have decreased ability to work. Annual medical expenditures increase by more than $4,000 for males who have had cancer and by nearly $3,300 for females.
Oncologists are helping their patients cope in a number of ways. For example, in the July issue of Cancer, a team of University of Chicago cancer specialists describe the first tool11 questions, assembled and refined from conversations with more than 150 patients with advanced cancer—to measure a patient’s risk for, and ability to tolerate, financial stress. The researchers named their patient-reported outcome measure COST (COmprehensive Score for financial Toxicity).
Lead author, Jonas de Souza, MD, said, “We need better ways to find out which patients are most at risk. Then we can help them get financial assistance. If patients know what to expect, they may want their physicians to consider less costly medications.”
Souza is a head and neck cancer specialist at the University of Chicago School of Medicine. Medication cost is the prime contributor to financial toxicity and at the recent 56th Annual Meeting of the American Society of Hematology (ASH) held this past December, an expert panel came together for a frank discussion about this aspect of cancer care. Hagop M. Kantarjian, MD, professor, department of leukemia, University of Texas MD Anderson Cancer Center, Houston, kicked off the discussion with a provocative talk about drug pricing, squarely identifying the pharmaceutical industry. Kantarjian went on to point out that high out-of-pocket costs of cancer treatments are leading patients to personal bankruptcy, adherence issues, and mental stress. See our coverage of the panel discussion, “Healthcare Costs in Need of Solutions: Experts at ASH Agree.”
References
- de Souza JA, Yap BJ, Hlubocky FJ, et al. The development of a financial toxicity patient-reported outcome in cancer: The COST measure.Cancer. 2014 Oct 15;120(20):3245-53.
- Mariotto AB, Yabroff KR, Shao Y, et al. Projections of the cost of cancer care in the United States:2010-2020.J Natl Cancer Inst. 2011;103:117-128.













