

|Articles|September 16, 2020
- The Expanding Continuum of Care in Metastatic Breast Cancer
Current Breast Cancer Landscape and Targeted Therapies for HER2 Overexpression
Breast cancer is the most common cancer that affects women, with estimates that it will account for 30% of all new cancer diagnoses in women in 2020. As the most commonly overexpressed receptor in breast cancer, HER2 is amplified or overexpressed in about 15% of breast cancers, leading to dysregulated cell proliferation. This article explores the current breast cancer landscape, with a focus on emerging HER2-targeted therapies, and discusses the unmet needs within the treatment landscape.
Advertisement
Breast cancer is the most common cancer that affects women, with estimates that it will account for 30% of all new cancer diagnoses in women in 2020.1 Among women in the United States, it is also the second leading cause of cancer-related death after lung cancer.1 In 2019, at least 3.8 million women in the United States had a history of past or current breast cancer and an estimated 268,600 new cases of invasive breast cancer were diagnosed.2 An additional 48,100 estimated new cases of ductal carcinoma in situ (DCIS) were diagnosed in 2019.2
With so many affected, it is important to provide women with treatment that eradicates local and regional disease and reduces the risk of metastatic recurrence.3,4 To this end, breast cancer is viewed as a group of diseases that are divided into 4 molecular subtypes based on the presence of biomarkers including estrogen receptor (ER), progesterone receptor (PR), and HER2.5 Molecular characterization provides useful information about prognosis and treatment decisions.6 Local and regional eradication can be achieved through surgery, and systemic therapy can reduce the risk of metastatic recurrence.3,4 After local treatment, different adjuvant therapies may be employed depending on the features of the tumor (eg, size, activity of lymph nodes, grade, ER/PR status, and HER2 status). Systemic therapies include endocrine therapy, chemotherapy, and targeted therapy. Standard endocrine therapies include tamoxifen or an aromatase inhibitor. Preferred chemotherapy regimens include doxorubicin/cyclophosphamide (AC) followed by paclitaxel, as well as docetaxel and cyclophosphamide. Preferred agents for HER2-targeted therapy include trastuzumab and pertuzumab.4
Despite the multitude of treatment options, there is still a great need to identify new pathways to target and to develop therapeutic agents for individuals who are unresponsive or are not candidates for standard therapies. After a brief overview of the disease and its subtypes, this review will discuss the standard and emerging therapeutic options, with a focus on targeted therapies for HER2 overexpression, and highlight the challenges and unmet needs within the treatment landscape.
Disease Overview and Prognosis
Breast cancer primarily affects women 50 years and older (82% of diagnoses), with diagnosis occurring at a median age of 62 years.2 The lifetime risk of diagnosis for women is 13% and about one-third of postmenopausal cases are associated with risk factors that may be modifiable, including postmenopausal obesity, hormone replacement therapy after menopause, sedentary lifestyle, alcohol use, and not breastfeeding.2,5 Other risk factors include genetic predisposition, a family history of breast cancer in a first-degree relative, early menarche (< 11 years), late menopause (≥ 55 years), late age at first pregnancy (> 30 years), mammographically dense breasts, and breast diseases such as DCIS, lobular carcinoma in situ, or atypical hyperplasia.5
The American Cancer Society (ACS) recommends regular screening by mammography for women with an average risk of breast cancer starting at age 45 years.7 Typically, early breast cancer does not have symptoms and it is diagnosed during routine screening.1 If there are symptoms, it is generally a painless lump that is noticed by the woman.1,5 On a mammogram, breast cancer appears as a calcification.8 If cancer is suspected, a core needle biopsy, or less commonly a surgical biopsy, is performed for microscopic analysis of the tissue.5 Other imaging techniques such as ultrasonography or MRI may also be used to further characterize the mass.8
The prognosis for breast cancer varies depending on the stage.2 Between 2009 and 2015, the 5-year overall survival (OS) rate was 98% for stage I, 92% for stage II, 75% for stage III, and 27% for stage IV.2 By race/ethnicity, survival is highest for Asian/Pacific Islanders and lowest for Blacks.2 Although the high survival rate for Asian/Pacific Islanders may be overestimated due to incomplete cancer registry data, racial disparities in survival rate are associated with a combination of factors including reduced access to prevention, detection, and treatment services, higher prevalence of health conditions such as obesity, and later stage at diagnosis.5 Prognosis also varies according to the molecular subtype (detailed below).
Biomarker Testing and Subtypes
Due to their clinical and prognostic utility of biomarkers, the American Joint Committee on Cancer and the National Comprehensive Cancer Network (NCCN) recommend testing breast cancer for them to determine if the disease is positive for HER2 (HER2 +) or for the hormone receptors (HRs) ER and PR.4,5,9 The levels of ER, PR, and HER2 are evaluated using immunohistochemistry. The sample is considered HR+ if ≥ 1% of cells are positive for ER and/or PR, and it is considered HER2 + if > 10% of cells exhibit intense staining.4,10,11
The 4 main molecular subtypes of breast cancer are triple negative, HR +/HER2-negative, HR + /HER2 +, and HR-negative/HER2 +.5 Triple-negative breast cancer (TNBC) is so termed because it is negative for ER, PR, and HER2.5 This subtype is more prevalent in women who have a BRCA1 gene mutation and is associated with a more aggressive clinical course, poorer prognosis, and a higher risk of relapse.5,12,13 The 5-year survival rate for TNBC is 77%.5 TNBC lacks a receptor target and thus chemotherapy is used for systemic adjuvant treatment.4,5,14 HR +/HER2-negative is the most common breast cancer.14 It is associated with a favorable prognosis (5-year survival rate of 92%) because this type grows slowly and is less aggressive.5 Systemic adjuvant treatment of these cancers usually involves endocrine therapy either alone or in combination with chemotherapy.4 HR +/HER2 + cancers account for about 10% of all breast cancers and are typically treated with a systemic adjuvant combination treatment consisting of endocrine therapy, chemotherapy, and a HER2-targeted therapy.4,14 HR +/HER2 + has a 5-year survival rate of 89%.5 HR-negative/HER2 + was historically the most aggressive of the subtypes but prognosis has improved to a 5-year survival rate of 83% with the advent of HER2-targeted therapies.5,9 This type is treated systemically with a combination of chemotherapy and targeted anti-HER2 therapy.4 HR-negative/HER2 + is the focus of the remainder of this review.
HER2+ Breast Cancer
HER2 is a tyrosine kinase receptor of the ErbB family and is associated with cell signaling pathways that lead to cell proliferation, differentiation, and inhibition of apoptosis.15 As the most commonly overexpressed receptor in breast cancer, HER2 is amplified or overexpressed in about 15% of breast cancers, leading to dysregulated cell proliferation.15-17 HER2 potently activates downstream pathways that are involved in tumor growth, thus its expression levels directly correlate with invasion and prognosis of breast cancer.18 For these reasons, HER2 has been employed as a molecular target for the development of new therapies over the last 20 years.18 Although HER2 + breast cancers grow faster and are more invasive than other types, they are generally responsive to anti-HER2 therapy, which has improved prognosis.5,18
Therapeutic Overview: Standards of Care and New Innovations in Therapy
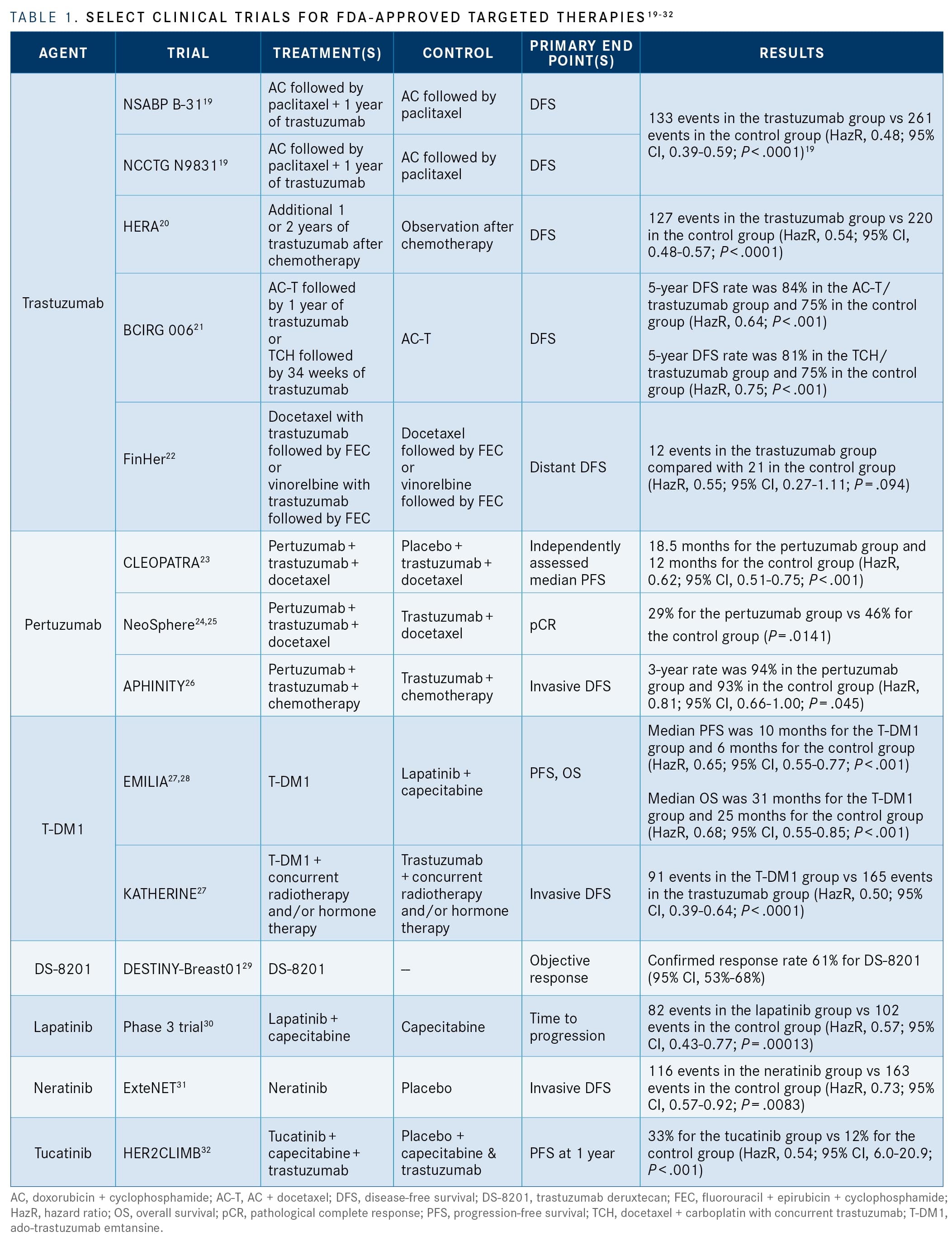
For patients with HER2 + breast cancer, HER2-targeted therapy is recommended. The preferred regimen is AC followed by paclitaxel with trastuzumab. Docetaxel, carboplatin, and trastuzumab (TCH) may also be used as a preferred regimen. Other regimens include AC followed by docetaxel and trastuzumab or docetaxel plus trastuzumab. Pertuzumab may also be incorporated into these adjuvant regimens if it was not used during neoadjuvant therapy. For metastatic breast cancer, the NCCN recommends pertuzumab plus trastuzumab in combination with a taxane (docetaxel or paclitaxel).4 Other regimens for metastatic breast cancer include ado-trastuzumab emtansine.4 Standard and other approved HER2-targeted therapies are discussed in more detail below, and the data for these agents are summarized in
.19-32
Trastuzumab
Trastuzumab (Herceptin; Genentech) is the foundation for treatment of HER2 + breast cancer. It is a humanized immunoglobulin G1 kappa monoclonal antibody (mAb) that was first approved by the FDA in 1998 and has been shown in several clinical trials to significantly improve disease-free survival (DFS) and OS.4,16,33 The National Surgical Adjuvant Breast and Bowel Project B-31 trial (NCT00004067) compared a chemotherapy regimen of 4 cycles of AC followed by weekly paclitaxel for 12 weeks with the same chemotherapy regimen plus 1 year of trastuzumab starting on the first day of paclitaxel treatment.19 The North Central Cancer Treatment Group N9831 trial (NCT00005970) compared 3 regimens: 4 cycles of AC followed by weekly paclitaxel for 12 weeks (group A), completion of the group A regimen followed by 1 year of trastuzumab, or completion of the group A regimen with 1 year of trastuzumab beginning on day 1 of paclitaxel therapy. The results of the B-31 and N9831 trials were analyzed together for a combined total of 1679 women in the control group and 1672 women in the trastuzumab group. The median follow-up was 2 years and individuals in the trastuzumab group had a higher rate of DFS compared with the control group (hazard ratio [HazR], 0.48; 95% CI, 0.39-0.59; P < .0001). Additionally, the risk of death was improved by about one-third (HazR, 0.67; 95% CI, 0.48 - 0.93; P = .015).19
The HERA trial (NCT00045032) was conducted in women who had received surgery and completed 4 cycles of adjuvant chemotherapy. After completion of this regimen, the study compared clinical observation alone (n = 1693) with an additional 1 year of trastuzumab (n = 1694) or 2 years of trastuzumab (n = 1694). After a median follow-up of 1 year, the combined 1-year and 2-year trastuzumab group had a higher rate of DFS compared with the observation group, with 127 DFS events occurring in the trastuzumab group compared with 220 in the observation group (HazR, 0.54; 95% CI, 0.43 - 0.67; P < .0001).20
In these studies, the use of adjuvant trastuzumab with anthracycline-based regimens (eg, doxorubicin) was associated with an increased incidence of congestive heart failure.19,20 Thus, the BCIRG 006 study additionally investigated a nonanthracycline, trastuzumab-based regimen (group 3) and compared 3 groups: 4 cycles of doxorubicin and cyclophosphamide followed by docetaxel (AC-T) every 3 weeks for 4 doses (group 1), AC-T followed by 1 year of trastuzumab starting with the first dose of docetaxel (group 2), and 6 cycles of docetaxel plus carboplatin with concurrent trastuzumab (TCH) followed by trastuzumab for 34 weeks. Both trastuzumab groups saw improvement in DFS and OS compared with the standard AC-T therapy. The 5-year rate of DFS for the AC-T plus trastuzumab group was 84% (HazR, 0.64; P < .001); OS was 92% (HazR, 0.63; P < .001). For TCH, the 5-year DFS rate was 81% (HazR, 0.75; P = .04) and OS was 91% (HazR, 0.77; P = .04). There was no statistical difference between the 2 trastuzumab groups; however, the BCIRG 006 study was not powered to compare them. The incidence of congestive heart failure was 5 times higher in the AC-T plus trastuzumab group compared with the TCH group (P < .001).21
The Finland Herceptin (FinHer) study (ISRCTN76560285) investigated the efficacy and safety of a brief course of a single chemotherapy agent coadministered with trastuzumab. Three cycles of docetaxel with or without trastuzumab followed by 3 cycles of fluorouracil, epirubicin, and cyclophosphamide (FEC) were compared with 3 cycles of vinorelbine with or without trastuzumab followed by FEC. Patients who were treated with trastuzumab tended to have improved DFS (HazR, 0.57; 95% CI, 0.33-0.99, P = .047). The brief course of trastuzumab and chemotherapy was not associated with a higher incidence of cardiac adverse events (AEs).22
Independent of ER status, the clinical trials with adjuvant trastuzumab have all demonstrated improvements to DFS that were clinically significant. Additionally, the B31, N9831, and Herceptin Adjuvant (HERA) trials also demonstrated clinically significant improvements in OS.4The most common AEs (≥ 5%) were headache, diarrhea, nausea, and chills.33
Pertuzumab
Pertuzumab (Perjeta; Genentech) is a recombinant humanized mAb that binds to HER2 and prevents it from forming a dimer with other HER receptors.25,34 Because pertuzumab binds HER2 at a different epitope than trastuzumab, it acts through complementary mechanisms to stimulate antibody-dependent cell-mediated cytotoxicity, and together pertuzumab plus trastuzumab have greater antitumor activity compared with either agent independently.25,34 Pertuzumab is indicated for use in combination with trastuzumab and docetaxel to treat patients with HER2 + metastatic breast cancer (MBC). It is also indicated in combination with trastuzumab and chemotherapy for adjuvant treatment of HER2 + early breast cancer with a high risk of recurrence, as well as for neoadjuvant therapy for HER2 + early, advanced, or inflammatory breast cancer.25
The efficacy and safety of pertuzumab were evaluated in multiple clinical trials. The CLEOPATRA trial (NCT00567190) was a phase 3 trial that compared pertuzumab plus trastuzumab plus docetaxel with a placebo and trastuzumab plus docetaxel to treat MBC.23 A clinically significant improvement in progression-free survival (PFS) was observed in the pertuzumab group (HazR, 0.62; 95% CI, 0.51 - 0.75; P < .001).23,25 For pertuzumab plus trastuzumab plus docetaxel, the most common grade 3-4 AEs were neutropenia, febrile neutropenia, leukopenia, diarrhea, peripheral neuropathy, anemia, asthenia, and fatigue.25
NeoSphere (NCT00545688) was a phase 2 trial that assessed the neoadjuvant activity of pertuzumab by comparing 4 groups: trastuzumab plus docetaxel, pertuzumab plus trastuzumab plus docetaxel, pertuzumab plus trastuzumab (no chemotherapy), and pertuzumab plus docetaxel.24,25 The combination of chemotherapy with both mAbs was more efficacious than chemotherapy with only 1 mAb. Compared with trastuzumab plus docetaxel alone, treatment with pertuzumab plus trastuzumab plus docetaxel resulted in significant improvement to pathological complete response (29% vs 46%; P = .0141).24 The most common grade 3-4 AEs in the NeoSphere trial were similar to those of the CLEOPATRA trial and included neutropenia, febrile neutropenia, leukopenia, and diarrhea.25
The APHINITY trial (NCT01358877) investigated the efficacy of adding pertuzumab to an adjuvant therapy of trastuzumab plus chemotherapy.26 Compared with placebo, adding pertuzumab significantly improved the 3-year rate of invasive DFS from 93% to 94% (HazR, 0.81; 95% CI, 0.66-1.00; P = .045).26 The most common grade 3-4 AEs included neutropenia, febrile neutropenia, diarrhea, decreased neutrophil count, anemia, decreased white blood cell count, leukopenia, fatigue, nausea, and stomatitis.25 The data from these clinical trials with pertuzumab demonstrate that it improves outcomes when used with trastuzumab.
Antibody-Drug Conjugates
Antibody-drug conjugates (ADCs) are composed of a recombinant mAb and a cytotoxic drug, bound by a synthetic link.35 The antibody binds to a specific marker on the surface of the cancer cell and is internalized. The drug is then released inside the cell to exert its cytotoxic effect.35
Ado-trastuzumab emtansine (T-DM1; Kadcyla; Genetech) is an ADC indicated to treat patients with HER2 + MBC who previously received trastuzumab and a taxane (separately or in combination). It is also indicated as an adjuvant treatment for patients who have residual invasive disease after neoadjuvant taxane and trastuzumab-based treatment for HER2 + early breast cancer.27 Its safety and efficacy were evaluated in 2 clinical trials: EMILIA (NCT00829166) and KATHERINE (NCT01772472).27,28 T-DM1 with lapatinib plus capecitabine in patients with metastatic HER2 + breast cancer who were treated previously with trastuzumab and a taxane chemotherapy agent were compared in the phase 3 EMILIA trial.28 Compared with the PFS for lapatinib plus capecitabine (6 months), treatment with T-DM1 significantly improved PFS to 10 months (HazR, 0.65; 95% CI, 0.55-0.77; P < .001).28 The KATHERINE trial assessed the safety and efficacy of T-DM1 in patients with HER2 + early breast cancer who had received neoadjuvant therapy with a taxane and trastuzumab. In addition to concurrent radiotherapy and/or hormone therapy, participants received either T-DM1 or trastuzumab. The invasive DFS at a median follow-up of 40 months showed a significant improvement for patients treated with T-DM1 compared with trastuzumab (12% vs 22%; HazR, 0.50; 95% CI, 0.39-0.64; P < .0001).27
Trastuzumab deruxtecan (DS-8201; Enhertu; Daiichi-Sankyo and AstraZeneca) is another ADC that consists of an anti-HER2 antibody conjugated to a topoisomerase inhibitor. It is indicated to treat adult patients with metastatic or unresectable breast cancer who have previously received 2 or more anti-HER2 treatments in the metastatic setting.36 In the phase 2 DESTINY-Breast01 trial (NCT03248492), DS-8201 was evaluated in patients with HER2 + metastatic or unresectable breast cancer and had already been treated with T-DM1. The confirmed response rate was 61% (n = 84) among patients who received the recommended dose of 5.4 mg/kg of DS-8201. The median PFS was 16 months (95% CI, 13 to not reached). The most common AEs (grade ≥ 3) were decreased neutrophil count, anemia, nausea, decreased white blood cell count, and fatigue.29
Kinase Inhibitors
A kinase inhibitor is a small molecule compound that binds to the ATP-binding domain of a tyrosine kinase receptor such as HER2. It therefore competes with ATP, which inhibits the enzyme’s phosphorylation activity.15
Lapatinib (Tykerb; Novartis) is a kinase inhibitor that binds to HER2 and to EGFR ErbB1, and inhibits growth stimulated by these pathways. A phase 3 trial evaluated the safety and efficacy of lapatinib in combination with capecitabine in patients with locally advanced or MBC that progressed after an initial treatment with anthracyclines, taxanes, or trastuzumab. Compared with capecitabine alone, lapatinib plus capecitabine lowered the risk of progression by 43% (HazR, 0.57; 95% CI, 0.43-0.77; P = .00013). The most common grade 3-4 AEs were diarrhea and palmar-plantar erythrodysesthesia syndrome. Lapatinib is indicated in combination with either capecitabine, for patients who received prior therapy with a taxane, anthracycline, or trastuzumab for HER2 + advanced or MBC; or with letrozole, to treat postmenopausal women with HR +/HER2 + MBC with an indication to receive hormone therapy.30
Neratinib (Nerlynx; Puma Biotechnology) is another kinase inhibitor that is indicated as a single agent for adjuvant treatment of HER2 + early breast cancer following adjuvant trastuzumab treatment. It is also indicated in combination with capecitabine to treat HER2 + advanced or MBC in adults who have previously received 2 or more anti-HER2 treatments.37 After a median follow-up of about 5 years, the results of the ExteNET phase 3 trial (NCT00878709) showed that patients who received neratinib rather than placebo after standard trastuzumab-based adjuvant therapy experienced significantly fewer invasive DFS survival events (HazR, 0.73; 95% CI, 0.57-0.92; P = .0083). For patients who received neratinib, the 5-year invasive DFS rate was 90% (95% CI, 88.3%-91.8%) vs 88%(95% CI, 85.7%-89.4%) for those who received placebo.31
Another kinase inhibitor, tucatinib (Tukysa; Seattle Genetics), was approved by the FDA in 2020 in combination with capecitabine and trastuzumab to treat unresectable or metastatic HER2 + breast cancer. This indication includes patients with brain metastases.38 In patients with HER2 + MBC who had already received treatment with trastuzumab, pertuzumab, and T-DM1, the HER2CLIMB trial (NCT02614794) evaluated tucatinib in combination with capecitabine and trastuzumab. Compared with the group treated with capecitabine and trastuzumab alone (n = 202), the tucatinib treatment group (n = 410) demonstrated a 46% lower risk of disease progression or death at 1 year (HazR, 0.54; 95% CI, 0.42-0.71; P < .001). For patients with brain metastases, this risk reduction was even greater at 52% (HazR, 0.48; 95% CI, 0.34-0.69; P < .001). The PFS at 1 year was favorable for the tucatinib treatment group at 33% compared with 12% for the placebo/combination group (HazR, 0.54; 95% CI, 6.0-0.9; P < .001). The most common AEs (grade ≥ 3) included palmar-plantar erythrodysesthesia syndrome, diarrhea, elevations in alanine aminotransferase and aspartate aminotransferase levels, and fatigue.32
Unmet Needs of HER2-Positive Breast Cancer
Although approved targeted therapies are effective to treat HER2 + breast cancer, there are still several challenges. The effectiveness of these targeted therapies is limited by the rapid development of resistance.16 Resistance develops through redundancy in signaling or alternative survival pathways that reactivate the HER2 pathway or its downstream signaling. These mechanisms include as follows39:
- activating compensatory pathways within the HER family such as HER3;
- activating other receptor tyrosine kinases or membrane receptors outside the HER family, such as insulin-like growth factor 1 receptor;
- hyperactivating the P13K/AKT/mTOR pathway through decreased levels of tumor suppressor genes such as PTEN or INPP4-B; and
- activating mutations in the PIK3CA gene for the catalytic subunit of phosphatidylinositol-4,5 bisphosphate 3-kinase.
Drug toxicity is another challenge for HER2 + breast cancer therapies. Trastuzumab and pertuzumab as well as ADCs that target HER2 are associated with cardiotoxicity that results in left ventricular cardiac dysfunction.25,27,33,36 Some trials, such as FinHer, have evaluated shorter courses of trastuzumab in order to limit cardiotoxicity, but the results from other trials have demonstrated that the standard 1-year course of trastuzumab yields greater benefits.22,40 Thus, cardiotoxicity persists as an important consideration with standard treatments for HER2 + breast cancer.
High per-patient costs pose another challenge to effective treatment of HER2 + breast cancer. The monthly cost of trastuzumab and pertuzumab are $4573 and $5673, respectively. Recent estimates indicate that the per-patient cost for an entire course of mAb treatment is $191,600. Although the estimated per-patient cost for a course of T-DM1 is lower, it is still high at $102,096.41 These costs may limit treatment access for patients in some demographic groups.
Emerging Therapeutics in HER2-Positive Breast Cancer
New therapies are in development to overcome resistance and improve toxicity. These include new mAbs, kinase inhibitors, ADCs, and immunotherapies. Agents that are being evaluated in phase 2 or 3 clinical trials are listed in
.42-74
Conclusions
Breast cancer is the most common cancer affecting women, and in 2019, at least 3.8 million women in the United States had a history of past or current breast cancer.1,2 It is usually diagnosed during screening by mammography, which starts at age 45 years as recommended by the ACS.1,7 A core needle biopsy is performed and the tissue is tested for biomarkers such as ER, PR, and HER2. Breast cancers that are positive for HER2 grow faster and are more invasive than other types. Prognosis for HER2 + breast cancer has improved due to the use of standard anti-HER2 therapies such as trastuzumab and pertuzumab. However, the development of resistance that reactivates the HER2 pathway or downstream signaling has limited the efficacy of targeted therapies against HER2. Additionally, these agents are associated with unfavorable drug toxicity and high costs. Thus, there is a great need to develop new drugs to overcome these challenges. Many agents such as anti-HER2 antibodies, kinase inhibitors, ADCs, and immunotherapies are currently being evaluated in phase 2 or 3 of clinical trials and are being investigated as novel therapies to treat HER2 + breast cancer.
Acknowledgment
Medical writing support was provided by Jessie Filer, PhD, and Kristen L. Phiel, MS, at PhiMed Communications, LLC.
References
1. Cancer facts & figures: 2020. American Cancer Society. 2020. Accessed August 17, 2020. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf
2. DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69(6):438-451. doi:10.3322/caac.21583
3. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321(3):288-300. doi:10.1001/jama.2018.19323
4. NCCN. Clinical Practice Guidelines in Oncology. Breast cancer, version 3.2020. Accessed July 23, 2020. https://www.nccn.org/professionals/physician_gls/default.aspx
5. Breast cancer: facts & figures, 2019-2020. American Cancer Society. 2019. Accessed August 17, 2020. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2019-2020.pdf
6. Van Poznak C, Somerfield MR, Bast RC, et al. Use of biomarkers to guide decisions on systemic therapy for women with metastatic breast cancer: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2015;33(24):2695-704. doi:10.1200/JCO.2015.61.1459
7. Oeffinger KC, Fontham ETH, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599-1614. doi:10.1001/jama.2015.12783
8. Alkabban FM, Ferguson T. Breast cancer. StatPearls/National Center for Biotechnology Information. Updated June 8, 2020. Accessed August 17, 2020. https://www.ncbi.nlm.nih.gov/books/NBK482286/
9. Amin MB, Edge S, Greene F, et al. eds. AJCC Cancer Staging Manual. 8th ed. The American College of Surgeons; 2017.
10. Rakha EA, Reis-Filho JS, Ellis IO. Combinatorial biomarker expression in breast cancer. Breast Cancer Res Treat. 2010;120(2):293-308. doi:10.1007/s10549-010-0746-x
11. Wolff AC, Hale Hammond ME, Allison KH, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline focused update. J Clin Oncol. 2018;36(20):2105-2122. doi:10.1200/JCO.2018.77.8738
12. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938-1948. doi:10.1056/NEJMra1001389
13. Liedtke C, Mazouni C, Hess KR, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26(8):1275-1281. doi:10.1200/JCO.2007.14.4147
14. Howlader N, Cronin KA, Kurian AW, Andridge R. Differences in breast cancer survival by molecular subtypes in the United States. Cancer Epidemiol Biomarkers Prev. 2018;27(6):619-626. doi:10.1158/1055-9965.EPI-17-0627
15. García-Aranda M, Redondo M. Protein kinase targets in breast cancer. Int J Mol Sci. 2017;18(12):2543. doi:10.3390/ijms18122543
16. Masoud V, Pagès G. Targeted therapies in breast cancer: new challenges to fight against resistance. World J Clin Oncol. 2017;8(2):120-134. doi:10.5306/wjco.v8.i2.120
17. Le Du F, Perrin C, Brunot A, et al. Therapeutic innovations in breast cancer. Presse Med. 2019;48(10):1131-1137. doi:10.1016/j.lpm.2019.04.005
18. Nami B, Wang Z. HER2 in breast cancer stemness: a negative feedback loop towards trastuzumab resistance. Cancers (Basel). 2017;9(5):40. doi:10.3390/cancers9050040
19. Romond E, Perez E, Bryant J, et al. Trastuzumab plus adjuvant chemotherpay for operable HER2-positive breast cancer. N Engl J Med. 2005;353(16):1673-1684. doi:10.1056/NEJMoa052122
20. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al; Herceptin Adjuvant (HERA) Trial Study Team. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353(16):1659-1672. doi:10.1056/NEJMoa052306
21. Slamon D, Eiermann W, Robert N, et al; Breast Cancer International Research Group. Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med. 2011;365(14):1273-1283. doi:10.1056/NEJMoa0910383
22. Joensuu H, Bono P, Kataja V, et al. Fluorouracil, epirubicin, and cyclophosphamide with either docetaxel or vinorelbine, with or without trastuzumab, as adjuvant treatments of breast cancer: final results of the FinHer Trial. J Clin Oncol. 2009;27(34):5685-5692. doi:10.1200/JCO.2008.21.4577
23. Baselga J, Cortes J, Kim S-B, et al; CLEOPATRA Study Group. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med. 2012;366(2):109-119. doi:10.1056/NEJMoa1113216
24. Gianni L, Pienkowski T, Im Y-H, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13(1):25-32. doi:10.1016/S1470-2045(11)70336-9
25. Perjeta. Prescribing information. Genentech; 2020. Accessed August 17, 2020. https://www.gene.com/download/pdf/perjeta_prescribing.pdf
26. von Minckwitz G, Procter M, de Azambuja E, et al; APHINITY Steering Committee and Investigators. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer. N Engl J Med. 2017;377(2):122-131. doi:10.1056/NEJMoa1703643
27. Kadcyla. Prescribing information. Genentech; 2019. Accessed August 17, 2020. https://www.gene.com/download/pdf/kadcyla_prescribing.pdf
28. Verma S, Miles D, Gianni L, et al; EMILIA Study Group. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med. 2012;367(19):1783-1791. doi:10.1056/NEJMoa1209124
29. Modi S, Saura C, Yamashita T, et al; DESTINY-Breast01 Investigators. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020;382(7):610-621. doi:10.1056/NEJMoa1914510
30. Tykerb. Prescribing information. Novartis Pharmaceuticals; 2018. Accessed August 17, 2020. https://www.novartis.us/sites/www.novartis.us/files/tykerb.pdf
31. Martin M, Holmes FA, Ejlertsen B, et al; ExteNET Study Group. Neratinib after trastuzumab-based adjuvant therapy in HER2-positive breast cancer (ExteNET): 5-year analysis of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2017;18(12):1688-1700. doi:10.1016/S1470-2045(17)30717-9
32. Murthy RK, Loi S, Okines A, et al. Tucatinib, trastuzumab, and capecitabine for HER2-positive metastatic breast cancer. N Engl J Med. 2020;382(7):597-609. doi:10.1056/NEJMoa1914609
33. Herceptin. Prescribing information. Genentech; 2018. Accessed August 17, 2020. https://www.gene.com/download/pdf/herceptin_prescribing.pdf
34. Franklin MC, Carey KD, Vajdos FF, et al. Insights into ErbB signaling from the structure of the ErbB2-pertuzumab complex. Cancer Cell. 2004;5(4):317-328. doi:10.1016/s1535-6108(04)00083-2
35. Beck A, Goetsch L, Dumontet C, Corvaïa N. Strategies and challenges for the next generation of antibody-drug conjugates. Nat Rev Drug Discov. 2017;16(5):315-337. doi:10.1038/nrd.2016.268
36. Enhertu. Prescribing information. Daiichi Sankyo; 2019. Accessed August 17, 2020. https://dsi.com/prescribing-information-portlet/getPIContent?productName=Enhertu&inline=true
37. Nerlynx. Prescribing information. Puma Biotechnology; 2020. Accessed August 17, 2020. https://nerlynx.com/pdf/full-prescribing-information.pdf
38. Tukysa. Prescribing information. Seattle Genetics; 2020. Accessed August 17, 2020. https://seagendocs.com/TUKYSA_Full_Ltr_Master.pdf
39. Pernas S, Tolaney SM. HER2-positive breast cancer: new therapeutic frontiers and overcoming resistance. Ther Adv Med Oncol. 2019;11:1758835919833519. doi:10.1177/1758835919833519
40. Puglisi F, Fontanella C, Amoroso V, et al. Current challenges in HER2-positive breast cancer. Crit Rev Oncol Hematol. 2016;98:211-221. doi:10.1016/j.critrevonc.2015.10.016
41. Tartari F, Santoni M, Pistelli M, Berardi R. Healthcare cost of HER2-positive and negative breast tumors in the United States (2012-2035). Cancer Treat Rev. 2017;60:12-17. doi:10.1016/j.ctrv.2017.08.005
42. Clinicaltrials.gov search results: HER2+ breast cancer, phase 2. Clinicaltrials.gov. Accessed August 11, 2020. https://clinicaltrials.gov/ct2/results?term=HER2%2B+breast+cancer&age_v=&gndr=&type=&rslt=&phase=1&Search=Apply
43. Clinicaltrials.gov search results: HER2+ breast cancer, phase 3. Clinicaltrials.gov. Accessed August 11, 2020. https://clinicaltrials.gov/ct2/results?term=HER2%2B+breast+cancer&age_v=&gndr=&type=&rslt=&phase=2&Search=Apply
44. Efficacy and Safety Study of ABP 980 Compared With Trastuzumab in Women With HER2-positive Early Breast Cancer (Lilac). ClinicalTrials.gov. Updated August 7, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT01901146
45. Study of Alpelisib (BYL719) in Combination With Trastuzumab and Pertuzumab as Maintenance Therapy in Patients With HER2-positive Advanced Breast Cancer With a PIK3CA Mutation. ClinicalTrials.gov. Updated July 24, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04208178
46. A Study To Evaluate the Efficacy and Safety Of Atezolizumab or Placebo in Combination With Neoadjuvant Doxorubicin + Cyclophosphamide Followed By Paclitaxel + Trastuzumab + Pertuzumab In Early Her2-Positive Breast Cancer (IMpassion050). ClinicalTrials.gov. Updated August 6, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03726879
47. The Efficacy and Safety of BAT8001 Injection for the Treatment of HER2-positive Advanced Breast Cancer. ClinicalTrials.gov. Updated December 4, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04185649
48. A Phase III Trial to Compare the Efficacy, Safety and Pharmacokinetics of HD201 to Herceptin in HER2+ Early Breast Cancer Patients (TROIKA). ClinicalTrials.gov. Updated April 15, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03013504
49. Margetuximab Plus Chemotherapy vs Trastuzumab Plus Chemotherapy in the Treatment of HER2+ Metastatic Breast Cancer (SOPHIA). ClinicalTrials.gov. Updated May 18, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT02492711
50. Study Evaluating The Effects Of Neratinib After Adjuvant Trastuzumab In Women With Early Stage Breast Cancer (ExteNET). ClinicalTrials.gov. Updated August 10, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT00878709
51. A Study of Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in Patients With HER2+ Metastatic Breast Cancer Who Have Received Two or More Prior HER2 Directed Regimens in the Metastatic Setting (NALA). ClinicalTrials.gov. Updated March 18, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT01808573
52. Randomized, Open Label, Clinical Study of the Targeted Therapy, Palbociclib, to Treat Metastatic Breast Cancer (PATINA). ClinicalTrials.gov. Updated October 30, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT02947685
53. A Study Of SIBP-01 Or CN-Trastuzumab Plus Docetaxel And Carboplatin In HER2 Positive Breast Cancer. ClinicalTrials.gov. Updated June 18, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03989037
54. Adjuvant Study of Pyrotinib in HER-2 Positive Breast Cancer (ATP). ClinicalTrials.gov. Updated February 5, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04254263
55. A Study of Evaluating The Effects Of Pyrotinib After Adjuvant Trastuzumab In Women With Early Stage Breast Cancer. ClinicalTrials.gov. Updated June 11, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03980054
56. Neoadjuvant Chemotherapy With Pyrotinib, Epirubicin and Cyclophosphamide Followed by Taxanes and Trastuzumab for HER-2+ Breast Cancer. ClinicalTrials.gov. Updated March 2, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04290793
57. Neoadjuvant Study of Pyrotinib in Combination With Trastuzumab in Patients With HER2 Positive Breast Cancer. ClinicalTrials.gov. Updated July 19, 2018. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03588091
58. Pyrotinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in Patients With HER2+ Metastatic Breast Cancer. (PHOEBE). ClinicalTrials.gov. Updated June 18, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03080805
59. Dual Blockage With Afatinib and Trastuzumab as Neoadjuvant Treatment for Patients With Locally Advanced or Operable Breast Cancer Receiving Taxane-anthracycline Containing Chemotherapy (DAFNE). ClinicalTrials.gov. Updated March 13, 2014. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT01594177
60. A Study of HER2+ Breast Cancer Patients With Active Brain Metastases Treated With Afatinib & T-DM1 vs. T-DM1 Alone (HER2BAT). ClinicalTrials.gov. Updated May 12, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04158947
61. Combination of AUY922 With Trastuzumab in HER2+ Advanced Breast Cancer Patients Previously Treated With Trastuzumab. ClinicalTrials.gov. Updated February 23, 2017. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT01271920
62. The AVIATOR Study: Trastuzumab and Vinorelbine With Avelumab OR Avelumab & Utomilumab in Advanced HER2+ Breast Cancer. ClinicalTrials.gov. Updated January 22, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03414658
63. Combination Study of BMS-754807 and Herceptin in Patients With Advanced or Metastatic Her-2-positive Breast Cancer. ClinicalTrials.gov. Updated July 13, 2012. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT00788333
64. Dendritic Cell Vaccines Against Her2/Her3, Cytokine Modulation Regimen, and Pembrolizumab for the Treatment of Brain Metastasis From Triple Negative Breast Cancer or HER2+ Breast Cancer. ClinicalTrials.gov. Updated August 18, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04348747
65. Clinical Study of Recombinant Anti-HER2 Humanized Monoclonal Antibody for Injection. ClinicalTrials.gov. Updated May 19, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04170595
66. KN035 in Combination With Trastuzumab and Docetaxel in HER2-positive Breast Cancer. ClinicalTrials.gov. Updated July 26, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04034823
67. Monalizumab and Trastuzumab In Metastatic HER2-pOSitive breAst Cancer: MIMOSA-trial (MIMOSA). ClinicalTrials.gov. Updated July 9, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04307329
68. Phase II Trial of Combination Immunotherapy With NeuVax and Trastuzumab in High-risk HER2+ Breast Cancer Patients (HER3+). ClinicalTrials.gov. Updated December 23, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT02297698
69. Niraparib in Combination With Trastuzumab in Metastatic HER2+ Breast Cancer. ClinicalTrials.gov. Updated July 13, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03368729
70. Impact of Pegfilgrastim on Trastuzumab Anti-tumor Effect and ADCC in Operable HER2+ Breast Cancer Breast Cancer (BREASTIMMU02). ClinicalTrials.gov. Updated April 21, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03571633
71. Ruxolitinib in Combination With Trastuzumab in Metastatic HER2 Positive Breast Cancer. ClinicalTrials.gov. Updated May 1, 2019. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT02066532
72. A Study of Neoadjuvant SHR6390 in Combination With Anastrozole, Pyrotinib, and Trastuzumab in Patients With ER+/HER2+ Breast Cancer. ClinicalTrials.gov. Updated January 22, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04236310
73. TPIV100 and Sargramostim for the Treatment of HER2 Positive, Stage II-III Breast Cancer in Patients With Residual Disease After Chemotherapy and Surgery. ClinicalTrials.gov. Updated July 29, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT04197687
74. A Study to Evaluate Concurrent VRP-HER2 Vaccination and Pembrolizumab for Patients With Breast Cancer. ClinicalTrials.gov. Updated May 5, 2020. Accessed August 26, 2020. https://clinicaltrials.gov/ct2/show/NCT03632941
Articles in this issue
Advertisement
Related Content
Advertisement





































{kind=link}
.jpg){kind=link}
Advertisement
Advertisement
Trending on Targeted Oncology - Immunotherapy, Biomarkers, and Cancer Pathways
1
Enfortumab Vedotin Plus Pembrolizumab Improves Survival in MIBC
2
FDA Grants Regular Approval to Rucaparib for BRCA-Mutated mCRPC
3
Teclistamab/Daratumumab Earns FDA Priority Voucher for R/R Myeloma
4
Early Relapse Guides Use of CAR T vs Other Options in LBCL
5