Cell-Free DNA Detection in Histiocytic Disorders May Transform Diagnosis and Treatment
Langerhans cell histiocytosis (LCH) and Erdheim-Chester disease (ECD) are characterized by a high frequency of BRAFV600E mutations, which are responsive to treatment with BRAF inhibitors such as vemurafenib.


Image: Memorial Sloan Kettering Cancer Center

Omar I. Abdel-Wahab, MD
Langerhans cell histiocytosis (LCH) and Erdheim-Chester disease (ECD) are characterized by a high frequency ofBRAFV600Emutations, which may occur in approximately 50% of patients with these diseases, and which are responsive to treatment with BRAF inhibitors such as vemurafenib.1-3Unfortunately, biopsy specimens from these conditions have a low proportion of histiocytes versus other cell types, such as stromal cells, and may be especially difficult to obtain because of the occurrence of histiocytic lesions in difficult-to-biopsy sites.1
Mutational analysis for both LCH and ECD thus entails significant challenges. Assessment of treatment response is also challenging, in view of the broad spectrum of anatomic sites and diverse types of lesions that may occur.1
In a report published December 2014 inCancer Discovery, coauthors David M. Hyman, MD, and Eli L. Diamond, MD, at Memorial Sloan Kettering Cancer Center (MSKCC), evaluated the utility of plasma and urine cell-free DNA (cfDNA), not only as a means to detect the presence of actionable mutations such asBRAFV600E, but also, for the first time, to detect dynamic changes in mutation burden during treatment for these conditions.
Omar I. Abdel-Wahab, MD, corresponding author on the paper, is an assistant in the Human Oncology and Pathogenesis Program (HOPP) and an attending physician on the Leukemia Service in the department of medicine at MSKCC.
“The impetus for this study,” he said, “was the consistent difficulty in identifying theBRAFV600Emutation in tissue biopsies from histiocytic disorder patients due to (1) heterogeneity in the cells infiltrating the tumors of these patients, and (2) frequent involvement in areas of the body that are difficult to biopsy and/or genotype in patients with these disorders, including bones and brain.”
He explained that the mutational testing on cfDNA was done in collaboration with Trovagene, Inc., incorporating droplet-digital polymerase chain reaction (PCR) and next-generation sequencing (NGS) technologies, and that the comparison of results from tissue-based genotyping with cfDNA genotyping was done in a blinded manner.
Describing the key findings of the study, Abdel-Wahab said, “In treatment-naïve patients, all patients whose tissue biopsy revealed theBRAFV600Emutation were identified as having the mutation in cfDNA (ie, 100% sensitivity). However, several patients whose tissue biopsy result was initially negative were actually revealed to have the mutation based on cfDNA analysis (which was confirmed by repeat tissue biopsy and mutational testing in all cases). This revealed that cfDNA analysis actually had improved sensitivity over tissue-based genotyping in histiocytic disorder patients.”
He also explained how the results demonstrated the similar specificity of both cfDNA and tissue genotyping, that cfDNA from both plasma and urine were analyzed, and that both gave 100% concordant results. The findings have obvious implications for ease of sampling versus conventional methods (eg, urine-based versus plasma-based sampling).
Asked how these findings might affect the treatment of patients with these rare disorders, Abdel-Wahab pointed to the promising efficacy of RAF inhibitors (ie, vemurafenib) in treating patients withBRAFV600E-mutant histiocytic disorder, as seen in results from an ongoing clinical trial (NCT01524978).4
“We repeated tissue biopsy genotyping on these patients with discordant tissue and cfDNA results to evaluate theBRAFV600Emutational status in the tissue. There was clear concordance of cfDNA and tissue biopsy genotyping results in these cases, and this allowed 2 patients to enroll on the clinical trial of vemurafenib who would have otherwise been ineligible to enroll on the study” (which required a tissue-based genotyping result revealing theBRAFV600Emutation).4
“In [the current] study, a tissue biopsy was unsuccessful in determining mutational status in 30% of patients, and was resolved in all patients by a liquid biopsy from urine and/or plasma. These data indicate the clinical utility of cell-free molecular diagnostics and how the incorporation of this new technology has immediate clinical application. The ease of collection for both plasma and urine samples over a tissue biopsy should pave the way for these less-invasive methods to correctly identify patients with these rare disorders for appropriate therapy selection,” Abdel-Wahab said.
Other results from the study detailed a longitudinal assessment ofBRAFV600EcfDNA burden. When comparing the ratio ofBRAFV600E/BRAF wild-type in cfDNA pretreatment, and following BRAF inhibitor therapy, inBRAFV600E-mutant patients, a significant decrease in the ratio was seen, indicating a progressive decrement in theBRAFV600Eallele burden (Figure 1;P< .0001).
Figure 1: Effect of therapy onBRAFV600Emutant allele burden in cell-free DNA (cfDNA) of systemic histiocytosis patients

 of systemic histiocytosis patients")
Effect of therapy on BRAFV600E mutant allele burden in cell-free DNA (cfDNA) of systemic histiocytosis patients
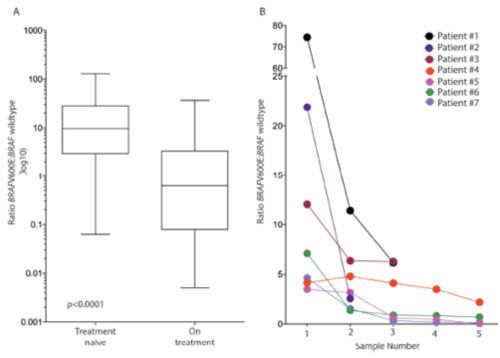
(A) Comparison of BRAFV600E allele burden in treatment-naïve urine samples compared with urinary samples acquired anytime during therapy. (B) Effect of RAF inhibitors on cfDNA BRAFV600E mutant allele burden in 7 consecutive patients treated with RAF inhibitors. The initial sample in each patient is prior to initiation of therapy.
Moreover, the decreases in allele burden over the course of the therapy were consistent with radiologic evidence of disease improvement. Conversely, an increase in allele burden, observed after the discontinuation of RAF inhibitor therapy (because of toxicity in one patient), was consistent with subsequent disease recurrence. Collectively, the findings indicate that such analyses could be used to proactively monitor patients’ response, or lack of response, to such therapies.
Regarding this second key finding of the study Abdel-Wahab noted, “This was the first study to demonstrate that RAF inhibitors actually reduce disease burden, in addition to reducing theBRAFV600Emutational burden in histiocytic disorders. What was quite unexpected was that immune-modulating therapies were also seen to reduce theBRAFV600Eallele burden when patients were efficaciously treated with these therapies instead of RAF inhibitors. We therefore think that cfDNA analysis for somatic mutations such as theBRAFV600Emutation may be used as a biomarker to track response to therapy in future studies of a wide array of therapies in histiocytic disorders. Cell-free DNA analysis will allow broader treatment applications than the traditional tissue biopsy because of the ease and frequency of the collection methods.”
Commenting further on the implications for future research, Abdel-Wahab noted another major unresolved issue in the histiocytic disordersidentifying clinically actionable mutations in the approximately 40% to 50% of patients who do not have theBRAFV600Emutations. He predicted that additional somatic mutations, in addition to theBRAFV600Emutation, will be identified using cfDNA analyses, citing, as an example, a single patient withoutBRAFV600Emutation who was shown to harbor aKRASmutation.
References
- Hyman DM, Diamond EL, Vibat CR, et al. Prospective blinded study of BRAFV600E mutation detection in cell-free DNA of patients with systemic histiocytic disorders [published online ahead of print October 16, 2014].Cancer Discov. . pii:CD-14-0742.
- Badalian-Very G, Vergilio JA, Degar BA, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis.Blood. 2010;116(11):1919-1923.
- Haroche J, Cohen-Aubart F, Emile JF, et al. Dramatic efficacy of vemurafenib in both multisystemic and refractory Erdheim-Chester disease and Langerhans cell histiocytosis harboring the BRAF V600E mutation.Blood. 2013;121(9):1495-1500.
- Clinicaltrials.gov. NCT01524978














