Hypertension Risk Among Cancer Patients Treated With Sunitinib: A Meta-analysis and Systematic Review
Sunitinib treatment is associated with a significantly increased risk of all-grade and high-grade hypertension.


Sungyub Lew, MD

Sungyub Lew, MD
Department of Surgery,
Saint Barnabas Medical Center, Livingston, New Jersey
Saint George’s University School of Medicine
Grenada, West Indies

Ronald S. Chamberlain, MD

Ronald S. Chamberlain,MD, MPA, FACS
Chairman and Surgeon-in-Chief, Department of Surgery
Saint Barnabas Medical Center, Professor of Surgery, New Jersey Medical School
Rutgers University
Livingston, New Jersey
Abstract
Purpose:Sunitinib is a multitargeted tyrosine kinase inhibitor widely used in cancer therapy that has been linked to varying degrees of treatment-related hypertension (HTN). The incidence and risk of HTN remain unclear. This study aims to assess the incidence and risk of sunitinib-associated HTN and provide a systematic review of sunitinib treatment.
Methods:A comprehensive literature search was completed of PubMed, Google Scholar, and the Cochrane Central Registry of Controlled Trials. Key words searched were: sunitinib, sutent, SU11248, cancer, and clinical trial. Eligible studies were limited to phase II and III trials of sunitinib, including safety reporting of HTN in patients with any type of malignancies. All clinical trials were analyzed for patient recruitment, intervention, and outcomes. Incidence and relative risk (RR) were calculated with 95% CI.
Results:62 single-arm or double-arm, phase II/III clinical trials involving 11,801 patients treated with sunitinib were identified. The incidence of sunitinib-associated all-grade and high-grade (grade ≥3) HTN was 19.3% (95% CI, 15.8-23.4) and 6.0% (95% CI, 4.6-7.8), respectively. Relative risk of sunitinib-associated allgrade and high-grade HTN was 3.13 (95% CI, 1.97-5.00;P<.001) and 2.44 (95% CI, 1.44-4.14;P= .001), respectively. Subgroup analysis demonstrated that the incidence and risk of severe sunitinib-associated HTN were not significantly different between 37.5-mg and 50-mg dosage regimens when monotherapy and/or concomitant chemotherapy were used, or by the type of malignancies, such as renal cell cancer, breast cancer, and non-small cell lung cancer.
Conclusion:Sunitinib treatment is associated with a significantly increased risk of all-grade and high-grade HTN.
Introduction
Sunitinib is an oral, multitargeted receptor tyrosine kinase inhibitor (TKI) that disrupts the signaling pathway activity against platelet-derived growth factor (PDGF) receptors α and β, vascular endothelial growth factor (VEGF) receptors 2 and 3, FMS-like tyrosine kinase-3 (FLT3), and c-KIT, all of which are involved in angiogenesis and tumor proliferation.1,2The US Food and Drug Administration (FDA) has approved sunitinib for treatment of advanced renal cell carcinoma (RCC), of gastrointestinal stromal tumor (GIST) after intolerance or disease progression on imatinib mesylate, and for progressive, well-differentiated pancreatic neuroendocrine tumors (pNETs) in patients with unresectable, locally advanced, or metastatic disease.3
Similar to other VEGF-receptor TKIs, sunitinib is associated with substantial adverse events (AEs).4-12These include hypertension (HTN), diarrhea, rash, fatigue, diarrhea, and mucositis.4,10-12In addition to these frequently reported AEs, previous studies with sunitinib therapy have reported an increased risk of developing hand-foot skin reaction, hematologic toxicities, arterial/venous thromboembolism, and hypothyroidism.5-9
A meta-analysis by Zhu et al found a significantly higher risk of HTN in patients given sunitinib compared with controls: relative risk (RR), 22.72; 95% CI, 4.48-115.29;P<.001.10The overall incidence of all-grade HTN was 21.6% (95% CI, 18.7-24.8) and of high-grade HTN was 6.8% (95% CI, 5.3-8.8). However, Zhu et al noted several limitations to their analysis, including an underestimation of the incidence of HTN associated with sunitinib because more than 70% of the patients included in the study were derived from the expanded access program, which did not include standardized toxicity data. Additionally, although the RR of high-grade HTN was significant, the findings were limited by the availability of very few randomized studies. The 1062 patients included in this analysis for the sunitinib arm and the 577 in the control arm came from only two randomized controlled trials, which had significant variation between them. Thus, the incidence and RR of high-grade HTN with sunitinib use have not yet been fully elucidated. Many additional randomized clinical trials have been completed since the previous meta-analysis, but with substantial variation in results. This study represents a meta-analysis of randomized controlled trials to assess the risk of high-grade HTN with sunitinib treatment and to provide a contemporary systematic review of sunitinib treatment.
Materials and Methods
Data Source
Data abstraction, meta-analysis, and systematic review have been performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,11and a comprehensive literature search of PubMed, Google Scholar, and the Cochrane Central Registry of Controlled Trials from January 1966 to August 2014 was conducted. Key words included in the search were: sunitinib, Sutent, SU11248, cancer, and clinical trial. The search was restricted to clinical trials in English. In case of duplicate publications, only the most recent and updated report of the clinical trial was included.
Study Selection, Data Extraction, and Clinical Endpoints
Clinical trials that met the following conditions were included in this study: (a) phase II or III trials in patients with cancer; (b) participants assigned to treatment with sunitinib; (c) events and sample size available for all-grade or high-grade HTN (grade 3 and 4); (d) participants assigned to treatment with only sunitinib at a dosage of either oral 25 mg, 37.5 mg, or 50 mg with either continuous daily dosing or intermittent treatment-free schedule; (e) safety reporting of all-grade or high-grade HTN available. To analyze the incidence of HTN associated with sunitinib, only trials with participants who were assigned to sunitinib as a monotherapy were used.
The incidence of HTN events in most of the included trials were recorded in accordance with Common Terminology Criteria for Adverse Events (CTCAE) version 3, which defines HTN as the following: (a) grade 1, asymptomatic, transient (<24 h) increase in blood pressure (BP) of >20 mm Hg (diastolic) or to >150/100 mm Hg if previously within normal limits, intervention not indicated; (b) grade 2, recurrent or persistent (>24 h) or symptomatic increase by >20 mm Hg (diastolic) or to >150/100 mm Hg if previously within normal limits, monotherapy might be indicated; (c) grade 3, requiring more than one drug or more intensive treatment than used previously; (d) grade 4, life-threatening consequences; and (e) grade 5, death.12
For RR analysis, randomized controlled trials were included in the study when participants were randomly assigned to sunitinib versus placebo, sunitinib plus best supportive care versus placebo plus best supportive care, or sunitinib plus concurrent immunotherapy and/or chemotherapy versus immunotherapy and/or chemotherapy alone. In case of crossover studies, only data available prior to crossover were used. If the data prior to crossing over were not available, the study was excluded.
Statistical Analysis
Incidence, RR, and 95% CIs for all-grade (grades 1-2) and high-grade (grades 3-4) HTN were calculated. Relative risk and CIs were calculated with data extracted only from randomized controlled studies, and the HTN events in patients assigned to sunitinib were compared with those assigned to control treatment in the same trial. To calculate 95% CIs, the variance of a log-transformed study-specific RR was derived using the delta method.
2
P
2
P
To calculate the incidence, clinical trials with sunitinib as a monotherapy were included in the analysis. The trials with concomitant chemotherapy and/or immunotherapy in addition to sunitinib were excluded from analysis to minimize the effect of other medications. The number of patients who developed HTN and the number of patients who received sunitinib were extracted from the selected single-arm and randomized controlled trials. The rate of AEs and 95% CIs were extracted from each trial. Traditional continuity corrections using a factor of 0.5 was adopted to calculate the RR and variance for the studies reporting zero events in any arm. In case of zero events in both groups, the RR was not calculable, and the study was excluded from the meta-analysis. Depending on the heterogeneity of included studies, fixed-effect or random-effects models were used for the calculation of RRs and summary incidence. Cochrane’s Q statistics with Istatistic was used to estimate statistical heterogeneity. An assumption of homogeneity was considered invalid forvalues <.05 or I>50%. When substantial heterogeneity was not observed, the pooled estimate was calculated based on the fixed-effect model. When significant heterogeneity was observed, the pooled estimate was calculated with a random-effects model. The publication bias regarding the primary endpoint (RR of high-grade HTN) was evaluated using Funnel plot, Begg’s test, and Egger’s test. A two-tailedvalue of <.05 was considered statistically significant. Statistical analysis was performed using the Comprehensive Meta-Analysis software Version 3 (Biostat, Englewood, New Jersey).
Results
Search Results
FIGURE 1
TABLE 1.
The search yielded 357 potentially relevant citations. The selection process excluded 295 citations; the reasons for study exclusion are detailed in. In all, 62 phase II and phase III clinical trials were considered eligible for the meta-analysis; 21 trials involved randomized treatment allocation, while 41 trials were single-arm trials. Of the 21 randomized treatment trials, 11 had placebo as a control and 10 had active treatment as the control arms. The HTN events in the included trials were reported in accordance with CTCAE version 2, 3, or 4. Two trials used version 2, 55 trials used version 3, two trials used version 4, and three trials did not specify the CTCAE version. The baseline characteristics of each trial are depicted in (Characteristics of All Sunitinib Clinical Trials Included in the Meta-analysis.Click here, to download PDF).
FIGURE 1. CONSORT diagram of selection process for the clinical trials.


CONSORT diagram of selection process for the clinical trials.
RCT indicates randomized control trial.
Overall Incidence of Hypertension
P
2
Only arms with sunitinib monotherapy were considered for the HTN incidence analysis. The trials that involved concomitant chemotherapy and/or immunotherapy were excluded because of the possibility of confounding effect on blood pressure from the concomitant therapy. A total of 4276 patients who were treated with sunitinib from both randomized and nonrandomized studies were included. All-grade HTN occurred in 807 of 3981 patients, 19.3% (95% CI, 15.8-23.4). The overall incidence of all-grade HTN was 3.7% (95% CI, 1.7-5.8) in the placebo arm. High-grade HTN occurred in 285 of 4276 patients, 6.0% (95% CI, 4.6-7.8). The overall incidence of high-grade HTN was 0.8% (95% CI, 0.0-1.7) in the placebo arm. In all-grade and high-grade HTN in sunitinib therapy, the heterogeneity test was significant (<.001 and I= 71%) and a random-effects model was used.
Relative Risk of Hypertension Events
For meta-analysis of the overall RR for all-grade and high-grade HTN events, 20 randomized clinical trials were included. The control arm was best supportive care or chemotherapy and/or immunotherapy. The treatment arm was sunitinib in addition to best supportive care or chemotherapy and/or immunotherapy. The RR of all-grade and high-grade HTN associated with sunitinib compared with control was 3.13 (95% CI, 1.97-5.00;P<.001) and 2.44 (95% CI, 1.44-4.14;P= .001), respectively (Click here, to download a PDF of FIGURES 2 and 3). A random-effects model was used for both all-grade and high-grade HTN because heterogeneity was found to be significant in both cases (P<.05 and I2 >50%).
Subgroup Analyses
Because of the potential risk of BP elevation from the use of concomitant chemotherapeutic or immunotherapeutic agents, the impact of the control arm on RR of high-grade HTN with sunitinib treatment was investigated. Among 20 randomized controlled trials, 10 involved sunitinib as a single agent and 10 used sunitinib in combination with chemotherapeutic and/or immunotherapeutic agents. The RR of high-grade HTN in combination therapy was 2.20 (95% CI, 1.00-4.88;P= .051) and was 3.01 in sunitinib monotherapy (95% CI, 1.34-6.75;P= .007). Although RR of high-grade HTN in combination therapy was not significant, there was no difference observed in the RR of high-grade HTN between sunitinib monotherapy and combination therapy (P = .588) (FIGURE 3). The incidence and RR of high-grade HTN were further investigated by malignancy type and by dosage regimen. The stratified malignancy types were RCC, breast cancer (BC), and non small cell lung cancer (NSCLC). There was no difference in the incidence of the high-grade HTN among the malignancies studied. There was no difference in the RR of high-grade HTN between RCC and non-RCC, between BC and non-BC, or between NSCLC and non- NSCLC. No differences in the RR of high-grade HTN were observed between a 37.5-mg dosage regimen and a 50-mg dosage regimen. The duration of therapy for 50-mg dosage regimen also showed no statistical difference whether treatment duration was shorter or longer than 4 months(TABLE 2).
TABLE 2. Incidence and Relative Risk of High-Grade HTN Stratified by Type of Malignancy Treated and by Treatment Regimen


Incidence and Relative Risk of High-Grade HTN Stratified by Type of Malignancy Treated and by Treatment Regimen
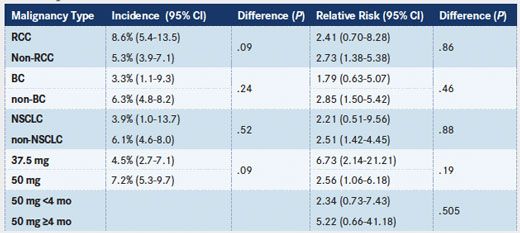
BC indicates breast cancer; NSCLC, nonsmall cell lung cancer; RCC, renal cell carcinoma.
Publication Bias
Publication bias for the all-grade HTN was significant via the Egger’s test (P<.001) but not the Begg’s test (P= .51). Regarding high-grade HTN, Egger’s test was significant (P<.001) but not Begg’s test (P= .54). Three trials compared sunitinib with the same VEGF class medications: bevacizumab,20pazopanib,76and sorafenib.25After adjusting for VEGF inhibitor class trials, publication bias was not observed for both all-grade and high-grade HTN: Begg’s test,P= .373, and Egger’s test,P= .288; Begg’s test,P= .322, and Egger’s test,P= .069, respectively.
Clinical Pearls
- All-grade and high-grade HTN occurs about 19% and 6% of patients, respectively, in sunitinib treatment.
- Sunitinib therapy increases the risk of HTN.
- Sunitinib-associated HTN does not differ by dosage regimen, by malignancy type, or when monotherapy and/or concomitant chemotherapy are used.
Discussion
Hypertension is a common adverse event observed in clinical trials associated with VEGF-inhibitor class medications. VEGF inhibitors, such as sunitinib, sorafenib, pazopanib, and bevacizumab have all been associated with increased risk of HTN.77In a recent meta-analysis, HTN developed in 23.6% (95% CI, 20.5-27.1) of patients treated with bevacizumab, 23.1% (95% CI, 19.3-26.9) of patients treated with sorafenib, and 35.9% (95% CI, 31.5-40.6) of patients treated with pazopanib.78-80
This study demonstrated that there was a high incidence of HTN associated with sunitinib therapy in patients with cancer: all-grade: 19.3% (95% CI, 15.8-23.4). Most HTN associated with sunitinib are grades 1 or 2, but high-grade HTN in association with sunitinib use is not infrequent (high-grade: 6.0% [95% CI, 4.6-7.8]). Chu et al studied 75 patients treated with sunitinib for GIST and reported that 8% of patients experienced congestive heart failure and more than 10% experienced a 28% reduction of left ventricular ejection fraction.81
VEGF-inhibitorinduced HTN is associated with decrease in nitric oxide (NO) production and endothelin signaling pathway activation.82Kruzliak et al described bioavailability of NO by direct inhibition of endothelial NO synthase through VEGFR-2 leading to reduced vasodilation, and NO-deficiencymediated cell proliferation in tunica media leading to fixation of HTN.83,84In addition, Wheeler et al has shown that treatment-associated HTN is related to interference in prostacyclin production in human umbilical endothelium cells.85The study by Robinson et al of urinary biomarkers from 80 patients with metastatic RCC showed the association between antiangiogenic therapy and suppression of metabolites of the NO pathway and cyclic guanosine monophosphate (cGMP).86
Hypertension is a dose-limiting toxicity in VEGF inhibitor therapy. However, there are no evidence-based guidelines for the management of VEGF inhibitor-induced HTN. Traditionally, most patients are managed with standard antihypertensive medications, and in the case of severe or persistent HTN, the VEGF inhibitor is temporarily or permanently discontinued until proper control of the HTN is achieved. Angiotensin-converting enzyme inhibitors have been most commonly used because proteinuria may also be associated with VEGF inhibitor use.87,88Because of the mechanism of VEGF inhibition, Kruzliak et al have suggested a possible role for long-acting NO donors such as molsidomine,83,84administered as a pretreatment 7 to 10 days before starting VEGF inhibitor therapy in patients whose baseline BP is ≥140/90 mm Hg or who have other cardiovascular risk factors. Further study is necessary to evaluate the benefit of pretreatment of NO donors in patients with pre-existing HTN treated with sunitinib.
In addition to managing VEGF-inhibitorinduced HTN, there is increasing evidence that elevation of blood pressure (BP) in patients who are on antiangiogenic therapy may predict better outcome. Rini et al investigated four studies of patients with metastatic RCC who were treated with sunitinib 50 mg daily on a 4-week-on, 2-week-off cycle. Patients with BP ≥140/90 had improved overall survival, progression-free survival, and hazard ratio for survival compared with patients who did not develop HTN after the sunitinib treatment.89Similar results were observed for bevacizumab, sorafenib, and apatinib as well.90-92Hypertension may reflect the effectiveness of the inhibition of VEGF-signaling pathway and tumor response.
In the current study, the risk of HTN did not vary by tumor type treated with sunitinib. Especially when the RR of developing high-grade HTN in RCC was high (RR = 2.41), it was not different from non-RCC (P= .86). In addition, this meta-analysis identified a lower risk of high-grade HTN (RR = 2.41) in patients treated with sunitinib compared with a previous study that reported high-grade HTN in patients with RCC with an RR as high as 8.20 (95% CI, 0.82-4.2).10Funakoshi et al78reported an increased incidence of HTN with the use of sorafenib in patients with RCC, but no significant increased RR of HTN in patients with RCC. A possible explanation for these discrepancies may be found in the current study data. One of the randomized controlled trials using sunitinib to treat RCC compared sunitinib with pazopanib, which are in the same class of VEGF inhibitors.28This trial was heavily weighted (45.63%), thereby strongly influencing the RCC subgroup analysis. The Funakoshi et al study also includes four randomized controlled trials comparing the same VEGF class of medications in patients with RCC. The dosing schedule or combination sunitinib therapy with other chemotherapy/immunotherapy agents have not been shown to increase the risk of high-grade HTN. The aforementioned trial of sunitinib versus pazopanib and other VEGF receptor TKIs may have some effect on these results as well.20,25,76
This study showed no difference in the risk of HTN by dosage regimen, but there were significant variations in the dosage intensity and treatment duration (Click here, to download FIGURE 5). The average dose varied from 18.8 mg/day to 37.5 mg/day. However, when the RR of high-grade HTN was compared by average dose per day with a cutoff of 30 mg/day, no difference in the risk was observed (P= .111). Additionally, the median treatment duration varied from 1.9 months to 11 months. When the trials were adjusted for treatment dosage and a median treatment duration cutoff of 4 months, no difference in the risk of high-grade HTN was observed for the 50-mg dosage regimen. The randomized trial by Motzer et al also showed no difference of the risk of high-grade HTN between 50 mg for 4 weeks followed by 2 weeks off cycle versus 37.5 mg continuous daily dosing regimen in patients with advanced RCC.93In their study, the 50-mg and 37.5-mg dosage groups were treated for median durations of 5 months and 6 months, respectively.
There are several limitations to the current meta-analysis. The incidence of HTN may have been underestimated in most of the trials, because 57 out of 64 used the CTCAE version 2 or 3 reporting system. In both versions 2 and 3, HTN is defined as BP >150/100 mm Hg or an increase in diastolic BP >20 mm Hg. This grading criterion can underestimate the incidence of HTN when compared with the Joint National Committee definition of HTN: BP >140/90 mm Hg. Also, the prevalence of the baseline HTN is not well described in most clinical trials and may overestimate new onset sunitinib-associated HTN. In this study, however, the estimated baseline incidence of all-grade (AG) HTN and high-grade (HG) HTN from the placebo arm were 3.7% and 0.8%, respectively. Finally, significant heterogeneity was observed in the study population, malignancy type, and treatment regimen.
In conclusion, our study suggests that the use of sunitinib is associated with significant risk of developing AG and HG HTN. The risk of HTN did not differ by type of malignancy treated, by dosage regimen, or when monotherapy or concomitant therapy was used. Early detection and effective management of HTN may allow more extensive use of sunitinib therapy and prevent possible cardiovascular complications.
REFERENCES
- Ikezoe T, Nishioka C, Tasaka T, et al. The antitumor effects of sunitinib (formerly SU11248) against a variety of human hematologic malignancies: enhancement of growth inhibition via inhibition of mammalian target of rapamycin signaling. Mol Cancer Ther. 2006;5(10):2522-2530.
- Ikezoe T, Yang Y, Nishioka C, et al. Effect of SU11248 on gastrointestinal stromal tumor-T1 cells: enhancement of growth inhibition via inhibition of 3-kinase/Akt/mammalian target of rapamycin signaling. Cancer Sci. 2006;97(9):945-951.
- Sutent [package insert]. New York: Pfizer Pharmaceutics Inc. http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/021938s13s17s18lbl.pdf. Accessed May 29, 2015
- Ibrahim EM, Kazkaz GA, Abouelkhair KM, Bayer AM, Elmasri OA. Sunitinib adverse events in metastatic renal cell carcinoma: a meta-analysis. Int J Clin Oncol. 2013;18(6):1060-1069.
- Chu D, Lacouture ME, Weiner E, Wu S. Risk of hand-foot skin reaction with the multitargeted kinase inhibitor sunitinib in patients with renal cell and non-renal cell carcinoma: a meta-analysis. Clin Genitourin Cancer. 2009;7(1):11-19.
- Funakoshi T, Latif A, Galsky MD. Risk of hematologic toxicities in cancer patients treated with sunitinib: a systematic review and meta-analysis. Cancer Treat Rev. 2013;39(7):818-830.
- Choueiri TK, Schutz FA, Je Y, Rosenberg JE, Bellmunt J. Risk of arterial thromboembolic events with sunitinib and sorafenib: a systematic review and meta-analysis of clinical trials. J Clin Oncol. 2010;28(13):2280-2285.
- Sonpavde G, Je Y, Schutz F, et al. Venous thromboembolic events with vascular endothelial growth factor receptor tyrosine kinase inhibitors: a systematic review and meta-analysis of randomized clinical trials. Crit Rev Oncol Hematol. 2013;87(1):80-89.
- Funakoshi T, Shimada YJ. Risk of hypothyroidism in patients with cancer treated with sunitinib: a systematic review and meta-analysis. Acta Oncol. 2013;52(4):691-702.
- Zhu X, Stergiopoulos K, Wu S. Risk of hypertension and renal dysfunction with an angiogenesis inhibitor sunitinib: systematic review and meta-analysis. Acta Oncol. 2009;48(1):9-17.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336-341.
- National Cancer Institute: Cancer Therapy Evaluation Program, Common Terminology Criteria for Adverse Events, Version 3.0, DCTD, NCI, NIH, DHHS. http://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf.
- Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368(9544):1329-1338.
- Motzer RJ, Hutson TE, Tomczak P, et al. Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma. J Clin Oncol. 2009;27(22):3584-3590.
- Barrios CH, Liu MC, Lee SC, et al. Phase III randomized trial of sunitinib versus capecitabine in patients with previously treated HER2-negative advanced breast cancer. Breast Cancer Res Treat. 2010;121(1):121-131.
- Mayer EL, Dhakil S, Patel T, et al. SABRE-B: an evaluation of paclitaxel and bevacizumab with or without sunitinib as first-line treatment of metastatic breast cancer. Ann Oncol. 2010;21(12):2370-2376.
- Socinski MA, Scappaticci FA, Samant M, Kolb MM, Kozloff MF. Safety and efficacy of combining sunitinib with bevacizumab + paclitaxel/carboplatin in non-small cell lung cancer. J Thorac Oncol. 2010;5(3):354-360.
- Wildiers H, Fontaine C, Vuylsteke P, et al. Multicenter phase II randomized trial evaluating antiangiogenic therapy with sunitinib as consolidation after objective response to taxane chemotherapy in women with HER2-negative metastatic breast cancer. Breast Cancer Res Treat. 2010;123(2):463-469.
- Raymond E, Dahan L, Raoul JL, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med. 2011;364(6):501-513.
- Robert NJ, Saleh MN, Paul D, et al. Sunitinib plus paclitaxel versus bevacizumab plus paclitaxel for first-line treatment of patients with advanced breast cancer: a phase III, randomized, open-label trial. Clin Breast Cancer. 2011;11(2):82-92.
- Bergh J, Bondarenko IM, Lichinitser MR, et al. First-line treatment of advanced breast cancer with sunitinib in combination with docetaxel versus docetaxel alone: results of a prospective, randomized phase III study. J Clin Oncol. 2012;30(9):921-929.
- Demetri GD, Garrett CR, Schoffski P, et al. Complete longitudinal analyses of the randomized, placebo-controlled, phase III trial of sunitinib in patients with gastrointestinal stromal tumor following imatinib failure. Clin Cancer Res. 2012;18(11):3170-3179.
- Scagliotti GV, Krzakowski M, Szczesna A, et al. Sunitinib plus erlotinib versus placebo plus erlotinib in patients with previously treated advanced non-small-cell lung cancer: a phase III trial. J Clin Oncol. 2012;30(17):2070-2078.
- Carrato A, Swieboda-Sadlej A, Staszewska-Skurczynska M, et al. Fluorouracil, leucovorin, and irinotecan plus either sunitinib or placebo in metastatic colorectal cancer: a randomized, phase III trial. J Clin Oncol. 2013;31(10):1341-1347.
- Cheng AL, Kang YK, Lin DY, et al. Sunitinib versus sorafenib in advancedhepatocellular cancer: results of a randomized phase III trial. J Clin Oncol. 2013;31(32):4067-4075.
- Crown JP, Dieras V, Staroslawska E, et al. Phase III trial of sunitinib in combination with capecitabine versus capecitabine monotherapy for the treatment of patients with pretreated metastatic breast cancer. J Clin Oncol. 2013;31(23):2870-2878.
- Curigliano G, Pivot X, Cortes J, et al. Randomized phase II study of sunitinib versus standard of care for patients with previously treated advanced triple-negative breast cancer. Breast. 2013;22(5):650-656.
- Motzer RJ, Hutson TE, Cella D, et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. 2013;369(8):722-731.
- Reni M, Cereda S, Milella M, et al. Maintenance sunitinib or observation in metastatic pancreatic adenocarcinoma: a phase II randomised trial. Eur J Cancer. 2013;49(17):3609-3615.
- Grivas PD, Daignault S, Tagawa ST, et al. Double-blind, randomized, phase 2 trial of maintenance sunitinib versus placebo after response to chemotherapy in patients with advanced urothelial carcinoma. Cancer. 2014;120(5):692-701.
- Heist RS, Wang X, Hodgson L, et al. CALGB 30704 (Alliance): A randomized phase II study to assess the efficacy of pemetrexed or sunitinib or pemetrexed plus sunitinib in the second-line treatment of advanced non-small-cell lung cancer. J Thorac Oncol. 2014;9(2):214-221.
- Michaelson MD, Oudard S, Ou YC, et al. Randomized, placebo-controlled, phase III trial of sunitinib plus prednisone versus prednisone alone in progressive, metastatic, castration-resistant prostate cancer. J Clin Oncol. 2014;32(2):76-82.
- Motzer RJ, Barrios CH, Kim TM, et al. Phase II randomized trial comparing sequential first-line everolimus and second-line sunitinib versus first-line sunitinib and second-line everolimus in patients with metastatic renal cell carcinoma. J Clin Oncol. 2014;32(25):2765-2772.
- Motzer RJ, Michaelson MD, Redman BG, et al. Activity of SU11248, a multitargeted inhibitor of vascular endothelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell carcinoma. J Clin Oncol. 2006;24(1):16-24.
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295(21):2516-2524.
- Saltz LB, Rosen LS, Marshall JL, et al. Phase II trial of sunitinib in patients with metastatic colorectal cancer after failure of standard therapy. J Clin Oncol. 2007;25(30):4793-4799.
- Kulke MH, Lenz HJ, Meropol NJ, et al. Activity of sunitinib in patients with advanced neuroendocrine tumors. J Clin Oncol. 2008;26(20):3403-3410.
- Rini BI, Michaelson MD, Rosenberg JE, et al. Antitumor activity and biomarker analysis of sunitinib in patients with bevacizumab-refractory metastatic renal cell carcinoma. J Clin Oncol. 2008;26(22):3743-3748.
- Faivre S, Raymond E, Boucher E, et al. Safety and efficacy of sunitinib in patients with advanced hepatocellular carcinoma: an open-label, multicentre, phase II study. Lancet Oncol. 2009;10(8):794-800.
- George S, Merriam P, Maki RG, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27(19):3154-3160.
- Hensley ML, Sill MW, Scribner DR, Jr, et al. Sunitinib malate in the treatment of recurrent or persistent uterine leiomyosarcoma: a Gynecologic Oncology Group phase II study. Gynecol Oncol. 2009; 115(3):460-465.
- Dror MM, Regan MM, Oh WK, et al. Phase II study of sunitinib in men with advanced prostate cancer. Ann Oncol. 2009;20(5):913-920.
- Carr LL, Mankoff DA, Goulart BH, et al. Phase II study of daily sunitinib in FDG-PET-positive, iodine-refractory differentiated thyroid cancer and metastatic medullary carcinoma of the thyroid with functional imaging correlation. Clin Cancer Res. 2010;16(21):5260-5268.
- Choong NW, Kozloff M, Taber D, et al. Phase II study of sunitinib malate in head and neck squamous cell carcinoma. Invest New Drugs. 2010;28(5):677-683.
- Feldman DR, Turkula S, Ginsberg MS, et al. Phase II trial of sunitinib in patients with relapsed or refractory germ cell tumors. Invest New Drugs. 2010;28(4):523-528.
- Koeberle D, Montemurro M, Samaras P, et al. Continuous Sunitinib treatment in patients with advanced hepatocellular carcinoma: a Swiss Group for Clinical Cancer Research (SAKK) and Swiss Association for the Study of the Liver (SASL) multicenter phase II trial (SAKK 77/06). Oncologist. 2010;15(3):285-292.
- Machiels JP, Henry S, Zanetta S, et al. Phase II study of sunitinib in recurrent or metastatic squamous cell carcinoma of the head and neck: GORTEC 2006-01. J Clin Oncol. 2010;28(1):21-28.
- Mackay HJ, Tinker A, Winquist E, et al. A phase II study of sunitinib in patients with locally advanced or metastatic cervical carcinoma: NCIC CTG Trial IND.184. Gynecol Oncol. 2010;116(2):163-167.
- O’Reilly EM, Niedzwiecki D, Hall M, et al. A Cancer and Leukemia Group B phase II study of sunitinib malate in patients with previously treated metastatic pancreatic adenocarcinoma (CALGB 80603). Oncologist. 2010;15(12):1310-1319.
- Shanafelt T, Zent C, Byrd J, et al. Phase II trials of single-agent anti-VEGF therapy for patients with chronic lymphocytic leukemia. Leuk Lymphoma. 2010;51(12):2222-2229.
- Sonpavde G, Periman PO, Bernold D, et al. Sunitinib malate for metastatic castration-resistant prostate cancer following docetaxel-based chemotherapy. Ann Oncol. 2010;21(2):319-324.
- Bellmunt J, Gonzalez-Larriba JL, Prior C, et al. Phase II study of sunitinib as first-line treatment of urothelial cancer patients ineligible to receive cisplatin-based chemotherapy: baseline interleukin-8 and tumor contrast enhancement as potential predictive factors of activity. Ann Oncol. 2011;22(12):2646-2653.
- Biagi JJ, Oza AM, Chalchal HI, et al. A phase II study of sunitinib in patients with recurrent epithelial ovarian and primary peritoneal carcinoma: an NCIC Clinical Trials Group Study. Ann Oncol. 2011; 22(2):335-340.
- Buckstein R, Kuruvilla J, Chua N, et al. Sunitinib in relapsed or refractory diffuse large B-cell lymphoma: a clinical and pharmacodynamic phase II multicenter study of the NCIC Clinical Trials Group. Leuk Lymphoma. 2011;52(5):833-841.
- Hui EP, Ma BB, King AD, et al. Hemorrhagic complications in a phase II study of sunitinib in patients of nasopharyngeal carcinoma who has previously received high-dose radiation. Ann Oncol. 2011;22(6):1280- 1287.
- Laurie SA, Gupta A, Chu Q, et al. Brief report: a phase II study of sunitinib in malignant pleural mesothelioma. the NCIC Clinical Trials Group. J Thorac Oncol. 2011;6(11):1950-1954.
- Mahmood ST, Agresta S, Vigil CE, et al. Phase II study of sunitinib malate, a multitargeted tyrosine kinase inhibitor in patients with relapsed or refractory soft tissue sarcomas. Focus on three prevalent histologies: leiomyosarcoma, liposarcoma and malignant fibrous histiocytoma. Int J Cancer. 2011;129(8):1963-1969.
- Neyns B, Sadones J, Chaskis C, et al. Phase II study of sunitinib malate in patients with recurrent high-grade glioma. J Neurooncol. 2011;103(3):491- 501.
- Novello S, Camps C, Grossi F, et al. Phase II study of sunitinib in patients with non-small cell lung cancer and irradiated brain metastases. J Thorac Oncol. 2011;6(7):1260-1266.
- Powles T, Kayani I, Blank C, et al. The safety and efficacy of sunitinib before planned nephrectomy in metastatic clear cell renal cancer. Ann Oncol. 2011;22(5):1041-1047.
- Schneider BJ, Gadgeel SM, Ramnath N, et al. Phase II trial of sunitinib maintenance therapy after platinum-based chemotherapy in patients with extensive-stage small cell lung cancer. J Thorac Oncol. 2011;6(6):1117-1120.
- Barrios CH, Hernandez-Barajas D, Brown MP, et al. Phase II trial of continuous once-daily dosing of sunitinib as first-line treatment in patients with metastatic renal cell carcinoma. Cancer. 2012;118(5):1252-1259.
- Chau NG, Hotte SJ, Chen EX, et al. A phase II study of sunitinib in recurrent and/or metastatic adenoid cystic carcinoma (ACC) of the salivary glands: current progress and challenges in evaluating molecularly targeted agents in ACC. Ann Oncol. 2012;23(6):1562-1570.
- Molina AM, Feldman DR, Ginsberg MS, et al. Phase II trial of sunitinib in patients with metastatic non-clear cell renal cell carcinoma. Invest New Drugs. 2012;30(1):335-340.
- Strosberg JR, Weber JM, Choi J, et al. A phase II clinical trial of sunitinib following hepatic transarterial embolization for metastatic neuroendocrine tumors. Ann Oncol. 2012;23(9):2335-2341.
- Tannir NM, Plimack E, Ng C, et al. A phase 2 trial of sunitinib in patients with advanced non-clear cell renal cell carcinoma. Eur Urol. 2012;62(6):1013-1019.
- Tong CC, Ko EC, Sung MW, et al. Phase II trial of concurrent sunitinib and image-guided radiotherapy for oligometastases. PLoS One. 2012;7(6):e36979.
- Yardley DA, Dees EC, Myers SD, et al. Phase II open-label study of sunitinib in patients with advanced breast cancer. Breast Cancer Res Treat. 2012;136(3):759-767.
- Barone C, Basso M, Biolato M, et al. A phase II study of sunitinib in advanced hepatocellular carcinoma. Dig Liver Dis. 2013;45(8):692-698.
- Han JY, Kim HY, Lim KY, et al. A phase II study of sunitinib in patients with relapsed or refractory small cell lung cancer. Lung Cancer. 2013;79(2):137-142.
- Ito T, Okusaka T, Nishida T, et al. Phase II study of sunitinib in Japanese patients with unresectable or metastatic, well-differentiated pancreatic neuroendocrine tumor. Invest New Drugs. 2013;31(5):1265-1274.
- Reynolds C, Spira AI, Gluck L, et al. Sunitinib malate in previouslyuntreated, nonsquamous, non-small cell lung cancer patients over the age of 70 years: results of a Phase II trial. Invest New Drugs. 2013;31(5):1330-1338.
- Chevreau C, Ravaud A, Escudier B, et al. A phase II trial of sunitinib in patients with renal cell cancer and untreated brain metastases. Clin Genitourin Cancer. 2014;12(1):50-54.
- Hutterer M, Nowosielski M, Haybaeck J, et al. A single-arm phase II Austrian/German multicenter trial on continuous daily sunitinib in primary glioblastoma at first recurrence (SURGE 01-07). Neuro Oncol. 2014;16(1):92-102.
- Jo JC, Hong YS, Kim KP, et al. A prospective multicenter phase II study of sunitinib in patients with advanced aggressive fibromatosis. Invest New Drugs. 2014;32(2):369-376.
- Motzer RJ, Hutson TE, Cella D, et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. 2013;369(8):722-731.
- Hamnvik OP, Choueiri TK, Turchin A, et al. Clinical risk factors for the development of hypertension in patients treated with inhibitors of the VEGF signaling pathway. Cancer. 2014.
- Funakoshi T, Latif A, Galsky MD. Risk of hypertension in cancer patients treated with sorafenib: an updated systematic review and meta-analysis. J Hum Hypertens. 2013;27(10):601-611.
- Ranpura V, Pulipati B, Chu D, Zhu X, Wu S. Increased risk of high-grade hypertension with bevacizumab in cancer patients: a meta-analysis. Am J Hypertens. 2010;23(5):460-468.
- Qi WX, Lin F, Sun YJ, et al. Incidence and risk of hypertension with pazopanib in patients with cancer: a meta-analysis. Cancer Chemother Pharmacol. 2013;71(2):431-439.
- Chu TF, Rupnick MA, Kerkela R, et al. Cardiotoxicity associated with tyrosine kinase inhibitor sunitinib. Lancet. 2007;370(9604):2011-2019.
- Robinson ES, Khankin EV, Karumanchi SA, Humphreys BD. Hypertension induced by vascular endothelial growth factor signaling pathway inhibition: mechanisms and potential use as a biomarker. Semin Nephrol. 2010;30(6):591-601.
- Kruzliak P, Kovacova G, Pechanova O. Therapeutic potential of nitric oxide donors in the prevention and treatment of angiogenesis-inhibitor-induced hypertension. Angiogenesis. 2013;16(2):289-295.
- Kruzliak P, Novak J, Novak M. Vascular endothelial growth factor inhibitorinduced hypertension: from pathophysiology to prevention and treatment based on long-acting nitric oxide donors. Am J Hypertens. 2014;27(1):3- 13.
- Wheeler-Jones C, Abu-Ghazaleh R, Cospedal R, Houliston RA, Martin J, Zachary I. Vascular endothelial growth factor stimulates prostacyclin production and activation of cytosolic phospholipase A2 in endothelial cells via p42/p44 mitogen-activated protein kinase. FEBS Lett .1997;420(1):28-32.
- Robinson ES, Khankin EV, Choueiri TK, et al. Suppression of the nitric oxide pathway in metastatic renal cell carcinoma patients receiving vascular endothelial growth factor-signaling inhibitors. Hypertension. 2010;56(6):1131-1136.
- Larochelle P, Kollmannsberger C, Feldman RD, et al. Hypertension management in patients with renal cell cancer treated with antiangiogenic agents. Curr Oncol. 2012;19(4):202-208.
- Kozloff MF, Berlin J, Flynn PJ, et al. Clinical outcomes in elderly patients with metastatic colorectal cancer receiving bevacizumab and chemotherapy: results from the BRiTE observational cohort study. Oncology. 2010;78(5-6):329-339.
- Rini BI, Cohen DP, Lu DR, et al. Hypertension as a biomarker of efficacy in patients with metastatic renal cell carcinoma treated with sunitinib. J Natl Cancer Inst. 2011;103(9):763-773.
- Bono P, Elfving H, Utriainen T, et al. Hypertension and clinical benefit of bevacizumab in the treatment of advanced renal cell carcinoma. Ann Oncol. 2009;20(2):393-394.
- Levy BI. Blood pressure as a potential biomarker of the efficacy angiogenesis inhibitor. Ann Oncol. 2009;20(2):200-203.
- Fan M, Zhang J, Wang Z, et al. Phosphorylated VEGFR2 and hypertension: potential biomarkers to indicate VEGF-dependency of advanced breast cancer in anti-angiogenic therapy. Breast Cancer Res Treat. 2014;143(1):141-151.
- Motzer RJ, Hutson TE, Olsen MR, et al. Randomized phase II trial of sunitinib on an intermittent versus continuous dosing schedule as first-line therapy for advanced renal cell carcinoma. J Clin Oncol. 2012;30(12):1371-1377.











Enhancing Precision in Immunotherapy: CD8 PET-Avidity in RCC
March 1st 2024In this episode of Emerging Experts, Peter Zang, MD, highlights research on baseline CD8 lymph node avidity with 89-Zr-crefmirlimab for the treatment of patients with metastatic renal cell carcinoma and response to immunotherapy.
Listen


Beyond the First-Line: Economides on Advancing Therapies in RCC
February 1st 2024In our 4th episode of Emerging Experts, Minas P. Economides, MD, unveils the challenges and opportunities for renal cell carcinoma treatment, focusing on the lack of therapies available in the second-line setting.
Listen

Conservative Management Is on the Rise in Intermediate-Risk Prostate Cancer
January 17th 2025In an interview with Peers & Perspectives in Oncology, Michael S. Leapman, MD, MHS, discusses the significance of a 10-year rise in active surveillance and watchful waiting in patients with intermediate-risk prostate cancer.
Read More

What Is Dark Zone Lymphoma, and Is It Clinically Relevant?
January 16th 2025Dark zone lymphoma includes aggressive B-cell lymphomas with shared molecular features. While some respond to escalated treatment, others remain resistant, highlighting the need for targeted approaches to improve outcomes.
Read More

